Short: The Futility of Most MRI Scans of the Shoulder and Knee in Those over 55
Most MRI scans in those over 55 years of age in the shoulder and knee show standard findings that make no difference to management or eventual outcome...so what really is their utility?
The Short Series
This is a new series that looks at interesting, new research and data that may not necessarily lead to any addition or subtraction to the 15-point guideline, but are issues worth knowing about or understanding from a larger healthspan/lifespan perspective.
The Book
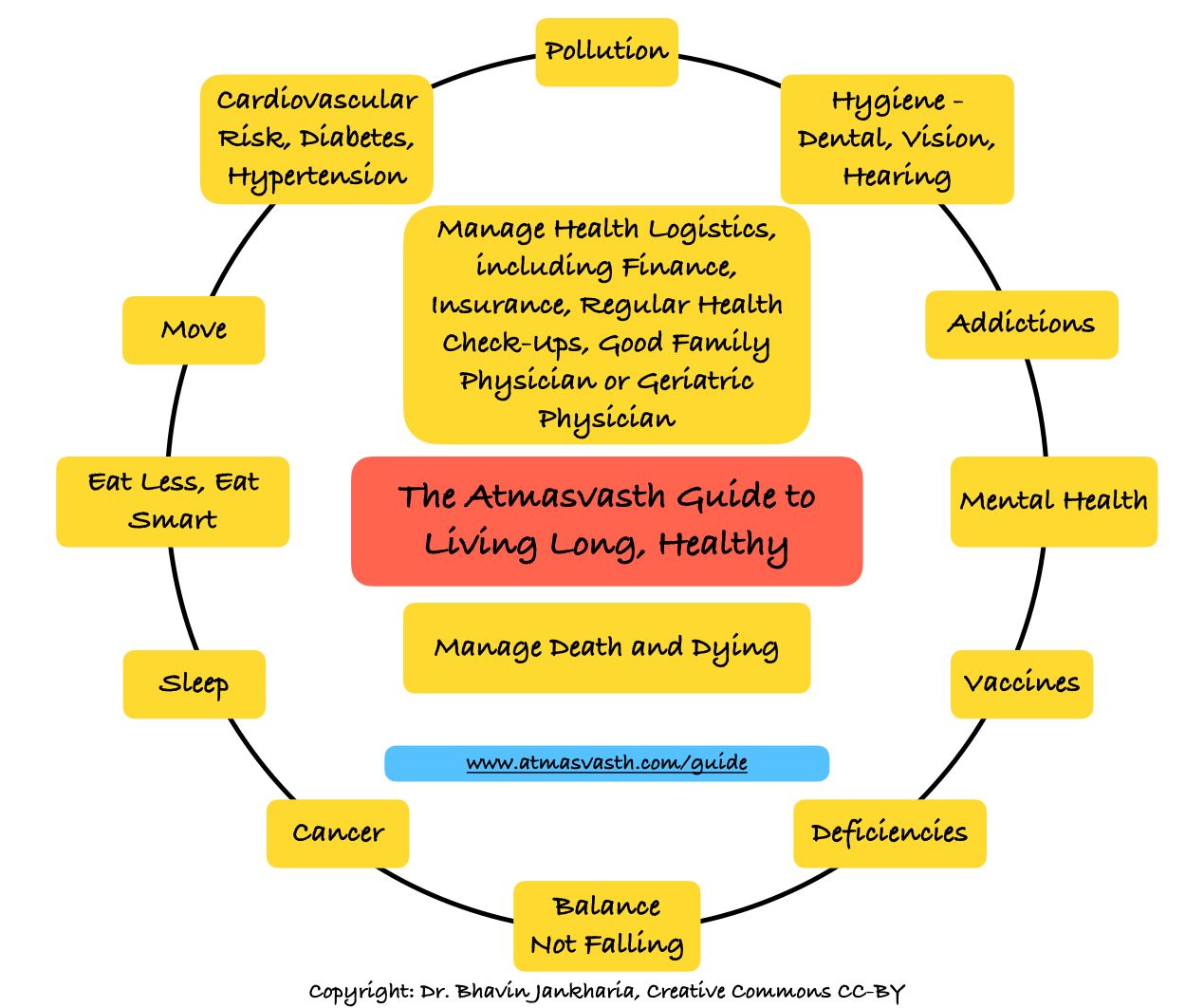
The Detailed 15-Point Guide to Live Long, Healthy
Audio
Soundcloud
YouTube
A YouTube version of the audio is also now available here.
Text
A 62-years old friend of mine who is very active, recently had progressive pain in the right shoulder. I asked him to show someone to get it checked, but he just wanted an MRI, which showed as expected, changes of frozen shoulder and some labral tears, none of which have any specific forms of treatment. The only things that help are a combination of exercise and physiotherapy.
When I interpret MRI scans of the knee and shoulder, I tell my fellows that there are 3 broad patient groups. The first are the young people with pain or trauma, where the MRI findings are important because they change management and guide therapy. Surgery and other interventions make a difference to the ability of these kids and young adults to get back to sports or just to normal daily life.
Then you have the middle-aged and elderly with acute injury, where too, the findings on MRI help with understanding what to do next. The most important is picking up fractures that have been missed on X-rays, especially impacted fractures of the greater tuberosity of the humerus or the proximal tibia of the knee.
The third group and the ones where whatever you report makes no difference to eventual outcomes is the chronic pain group of elderly people above the age of 55 who have degenerative disease or osteoarthritis, where there will be a laundry list of findings - in the shoulder, signs of adhesive capsulitis (fancy name for frozen shoulder), rotator cuff tears and/or labral tears - in the knee, cartilage loss, loose bodies, meniscal tears, some marrow edema and ACL mucoid degeneration. There are no interventions that help apart from muscle building and being active and mobile. In the shoulder, people get all sorts of injections and varying types of physiotherapy but eventually, things settle down if you give the shoulder enough time.
Because the knee is weight bearing, things don’t usually settle down even with injections and physiotherapy. What works is building the quadriceps and hamstrings to offload the knee and being as active as possible, but since the vast majority of people refuse to change their life-style, they all eventually progress to a total knee replacement.
The vast majority of MRIs of the knee and shoulder in the middle aged and elderly are pointless. Thirty-five years ago when we started doing MRIs, it was tough convincing orthopedic surgeons to refer patients for MRIs of the knee and shoulder because they trusted their clinical skills over the MRI findings. Now, people and patients want MRIs and if their orthopedic surgeons and nowadays physiotherapists only use clinical skills and do not ask for an MRI, they change doctors. This creates a vicious self-fulfilling prophecy - people and patients demand the scan to feel heard and doctors order it to avoid being seen as dismissive.
There is a lovely article in JAMA Internal Medicine published recently, from Finland where they did MRIs of the shoulders in symptomatic and asymptomatic individuals and found that rotator cuff abnormalities were found in 96% of asymptomatic and 98% of symptomatic individuals. In short: if you are of a certain age, your chance of having a 'finding' is nearly 100%. The MRI doesn't identify the cause of pain; it simply confirms you are aging and perhaps then it is just a good idea to call these age-related changes rather than abnormalities and the treating doctor could just assume a rotator cuff problem in every patient who comes to them and just manage them accordingly.
Unless the MRI finding is going to change treatment significantly and that generally means arthroscopy or surgery, which in most instances in the middle-aged and elderly are not indicated, what is the point of the MRI? Yes, there will always be a few elderly patients who will benefit from the MRI, especially if there are other clinical issues or significant injury as I mentioned earlier, but in the vast majority of patients who only present with chronic pain, the MRI does not change the eventual outcome.
The same is true of spine MRIs in the elderly, but I will talk about that some other time.
What does this mean for you and me? If you are over 55 and you have chronic pain in the shoulder and knee, sometimes with acute flare-ups, doing an MRI is not going to be make any difference to your treatment, over an X-ray, unless there is a specific reason to do the MRI, and the findings will make a big difference to the treatment over and above rest and physiotherapy and building muscle, etc.
You could ask your treating doctor a simple question, “Will the MRI make a difference?”. If the answer is maybe or no, you could perhaps avoid one.

The flip side is that MRIs in India cost so less (from Rs. 1500 at low cost centres to Rs. 9000 in premium institutes with high-end machines), and the barrier to getting one done is so low that sometimes it is simpler to get one done than get into a Q & A with your doctor. It is for you to decide...resisting unnecessary testing vs going with the flow.
Footnotes
1. Ibounig T, Järvinen TLN, Raatikainen S, Härkänen T, Sillanpää N, Bensch F, et al. Incidental Rotator Cuff Abnormalities on Magnetic Resonance Imaging. JAMA Intern Med. 2026 Feb 16. doi:10.1001/jamainternmed.2025.7903
{kind=link}
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.