Nobody is Coming to Save You
Why where you live in India decides whether you survive a heart attack, stroke, or fall — and what you can plan for today.

Audio and YouTube versions available at the end of this email.
A few weeks ago, at a wedding in Lonavala, an elderly guest had slurred speech and weakness and a possible diagnosis of stroke. The family was well-off, two of them doctors, but it still took over an hour to decide what to do (local Lonavala vs Mumbai) and then for the ambulance to come…finally the patient was shifted to Mumbai and luckily it wasn’t a stroke but heart failure, but a lot of time was lost in just dithering about decisions.
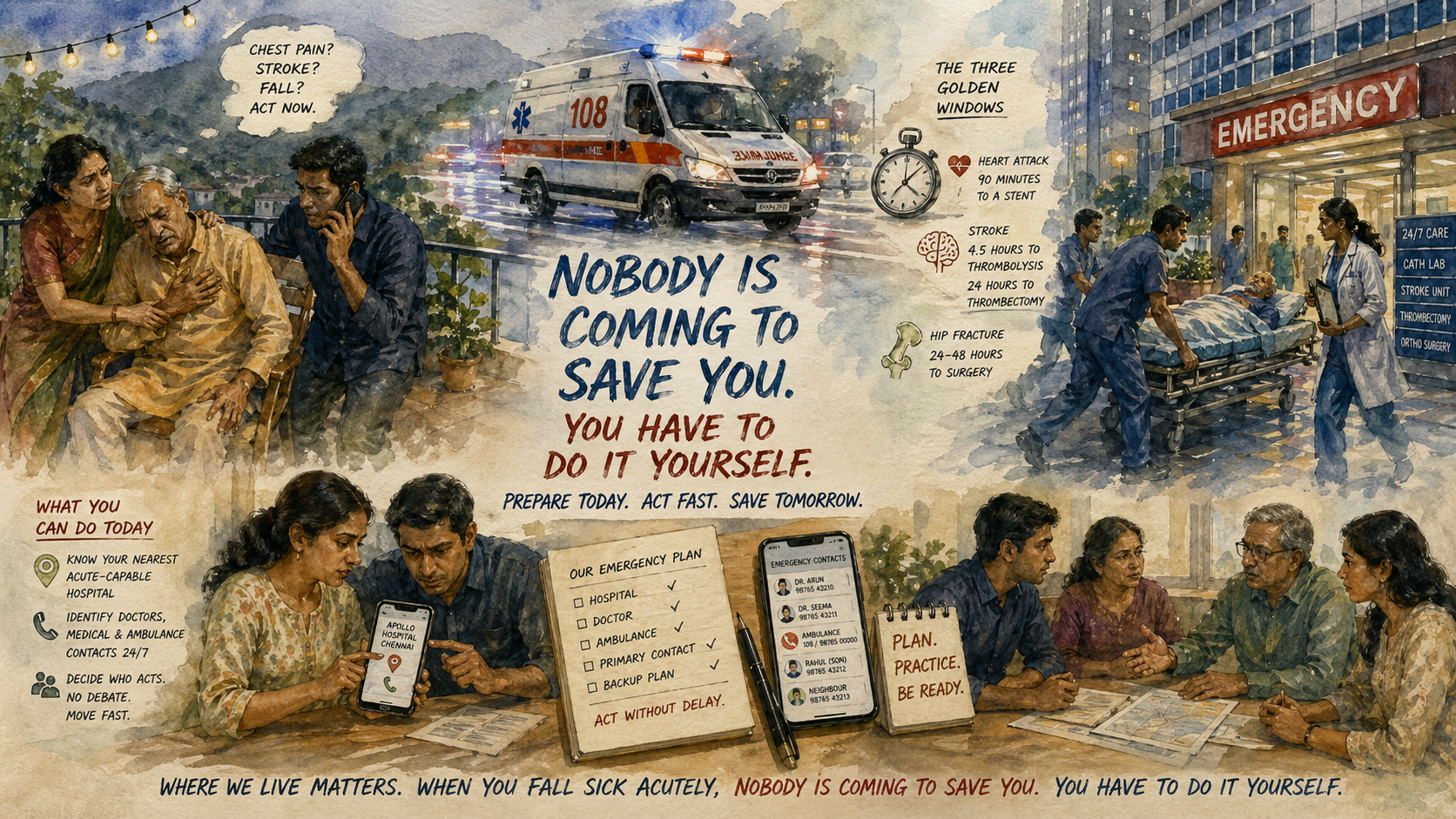
The Three Golden Windows
Almost everything we do in our atmasvasth quest to live long, healthy is aimed at not having a heart attack, a stroke, not falling and fracturing, not getting a cancer and not getting dementia. But, despite everything we do correctly, if one of these acute things does happen (stroke, heart attack, fracture, especially hip), there is a second, entirely separate question that decides your outcome: how quickly can you get to the right hospital, with the right equipment, and the right specialist?
For three of the big emergencies, medicine has settled on specific time windows, which if missed lead to poorer outcomes and sometimes even death.
Heart attack — 90 minutes to a stent. The gold standard for an acute heart attack with ST-elevation (STEMI infarct) is primary percutaneous coronary intervention (PCI), which is a catheter-based procedure to open the blocked artery. The benchmark that every Western health system is measured against is "first medical contact to balloon" in under 90 minutes. Every minute of delay beyond that leads to irreversible destruction of heart muscle and eventually a reduced healthspan and lifespan.
Stroke — 4.5 hours to thrombolysis, 24 hours to thrombectomy. For an ischemic stroke, which is the most common type of stroke, thrombolytic drugs must be given within 4.5 hours of the onset of paralysis. Mechanical thrombectomy, where a clot is physically pulled out of a brain artery, has a window of up to 24 hours but works best in the first 6. After these windows, the brain tissue is dead, and no intervention can bring it back.
Hip fracture — 24 to 48 hours to surgery. For an elderly person with a femoral neck fracture, outcomes — mortality, return to walking, independence — are measurably worse if surgery happens after 48 hours… ideally it should be within 24.
These are not aspirational numbers. They are the standard of care everywhere a modern health system exists.
What the West Actually Delivers
In the United States, 98% of the population lives within reach of a hospital that can deliver PCI within 90 minutes of first medical contact [1]. The way this works is simple and, from an Indian perspective, almost unimaginable. A person gets chest pain. They, or someone near them, dials 911. An ambulance with trained paramedics arrives within minutes. An ECG is done in the ambulance and transmitted ahead. The cath lab is activated before the patient reaches the hospital. By the time the patient rolls in, the interventional cardiologist is scrubbed and waiting.
The UK, Sweden, Germany, Japan, Australia — all run versions of this. Stroke networks work the same way. Hip fractures are on fast-track pathways in every major hospital in the NHS, where the 48-hour-to-surgery target is an audited performance indicator.
None of this exists in India. Not for the middle class. Not for the rich. Not for anyone.
What India Actually Delivers
There is no 911 or national emergency medical service (EMS). There are private ambulance services of wildly variable quality in big cities, and effectively nothing outside them. The state-run 108 service exists but is overstretched and often slow. Traffic is unpredictable. Most ambulances do not carry paramedics who can diagnose and pre-treat a heart attack en route. Most hospitals do not have 24/7 cath lab activation. Most hospitals in India — more than 90% — cannot handle an acute stroke around the clock, simply because there are not enough trained interventional neuroradiologists and neurologists in the country.
The data bears this out. In a large Indian stroke registry published this year, Mathur and colleagues found that only 20% of stroke patients presented to a hospital within 4.5 hours, while 38% presented after 24 hours [2]. Only 4.6% received thrombolysis. Only 0.7% received thrombectomy.
For heart attacks, STEMI India's hub-and-spoke program in Tamil Nadu [3] is the best-organized network in the country, and even there, the achievement is getting thrombolysis — which is the backup treatment — into district hospitals in a usable time. Primary PCI within 90 minutes is simply not the operational target, because it is not feasible for most of the country.
For hip fractures, the Armstrong study [4] found that only 56% of Indian patients with a fall and hip fracture reached a hospital within 24 hours. Even after admission, 62% had surgery only after 72 hours. Wealth does not fix this either. In private Indian hospitals, even with money no object, the average time from admission to hip surgery is around three days — because of pre-operative workups, cardiac clearances, anaesthesia consults, and the general leisureliness of non-emergency scheduling. I have seen breast cancer diagnoses go from biopsy to surgery in 72 hours at the same hospitals…a breast cancer that has been growing for two years does not need to be operated on immediately. A hip fracture does.
Why Money Does Not Solve This
In Western countries, wealth and poverty affect many things — which neighborhood you live in, what insurance you have, whether you go bankrupt paying for care — but they do not meaningfully affect whether an ambulance reaches you in fifteen minutes and takes you to a PCI-capable hospital. That infrastructure is a public good, paid for collectively, and it shows up for everyone.
In India, no amount of private wealth substitutes for the missing public infrastructure. You can own the most expensive bungalow in Lonavala, and it will not conjure an interventional neurologist into being there at 2 am. You can have the best health insurance in the country, and it will not shorten the forty-minute drive to the nearest cath lab. There is no air ambulance network with helicopters on standby. The few air ambulance services that exist are fixed-wing, require hours of notice, and cannot land near most towns.
The richest people in Lonavala, Ranchi, Goa, Alibaug are in a worse position during an acute medical emergency than a middle-class person living a ten-minute walk or drive from Hinduja Hospital in Mahim, or from Apollo in Chennai, or from Medanta in Gurgaon. And all of them — rich or middle-class, Mumbai or Lonavala — are in a worse position than an average person in Stockholm or Manchester or Minneapolis.
What You Can Actually Do
Accepting that this is the system we live in, the question becomes: what can you do, as an individual, to maximise the chance that you or a family member actually gets treatment inside the golden window?
1. Know your nearest acute-capable hospital. Today. Before anything happens. For yourself and your near and dear ones. Not the nearest hospital. Not the nicest-looking hospital. The nearest hospital that can do, 24/7, the specific things you might need: primary PCI, stroke thrombolysis and thrombectomy, and acute orthopedic surgery. These are three different capabilities and not every hospital has all three. Find this out now. Visit the hospital's website, call, ask a doctor friend and save the address and the route in your phone. Do this for yourself and your near and dear ones.
2. Identify a doctor, a medical service, an ambulance service or a contact who is available 24/7. This is not easy, but if possible and if available, make sure you have the names and numbers of nearby doctors or doctor services that can be contacted 24/7 and can pre-activate everything for you…from seeing you or advising you, getting the ambulance to you fast and getting the hospital activated for you. If none of these are available, at least make sure you have the numbers of ambulances that can be called at short notice and if even that is a problem, then some person who will get out of bed instantly and rush to your aid.
3. Decide, in advance, who acts. The single biggest predictor of whether someone gets to hospital in time is whether the person around them moves without debate. Have this conversation with your spouse, your adult children, your parents — if this happens, the plan is not up for discussion.
What Does this Mean for You and Me?
Everything we do…physical activity, eating sensibly, sleeping well, controlling high blood pressure, lipid levels, high blood sugar, not smoking, taking vaccines and being careful about our surroundings…is useless if we land up with a heart attack, stroke or fracture and then can’t get to a hospital in time to get treated.
You need to have your logistics sorted out in advance…which hospital to go to, which doctor to call, which ambulance service to dial and who among your near and dear ones to lean on if and when this happens. This is not just for heart attacks, strokes and fractures, but also if you have acute abdominal pain that does not settle with medicines, acute breathlessness, sudden blindness…anything acute that sets off alarms in you or those around you.
During the Lonavala incident, the family should have known who to connect with, which hospital to go to, activated the ambulance pick-up instantly and moved out to the right hospital within minutes, not hours. If it had turned out to be a stroke, valuable time would have been wasted because of this poor preparation and decision making.
Where we live matters. And when you fall sick acutely, nobody is coming to save you. You have to do it yourself.
This piece adds to the 14th point in the Atmasvasth guide to live long, healthy, which is:
14. Identify doctors and health systems around you and work out the associated health and disease logistics in advance. This is a one-time exercise, and includes:
Identify a good family physician to help you navigate the system if you fall ill.
Identify a health coach who can do the same.
Be aware of acute conditions where speed is important and of non-acute conditions where you have to think calmly and move slowly.
Know the names and contact numbers of physicians, hospitals, ambulances and people you can contact in acute situations. Write them in this book or have them easily available for your near and dear ones.
Listening Options
Audio File
YouTube
Footnotes
1. Koka A. America Has Solved the Hardest Healthcare Access Problem Better Than Anyone Else — Here's the Data. https://anishkokamd.substack.com/p/the-us-healthcare-system-has-basically
2. Mathur P, Huliyappa D, Pv P, et al; National Stroke Registry Programme (NSRP) Investigators. Stroke patterns, risk factors, management, and outcomes from hospital-based stroke registries in India. Int J Stroke. 2026 Jan 7. PMID: 41502107.
3. Mullasari AS, Victor SM, Alexander T. STEMI India: reimagining STEMI networks in low- and middle-income countries. AsiaIntervention. 2022 Mar;8(1):17-23. PMID: 35350796.
4. Armstrong E, et al. [Global hip fracture outcomes study, as cited in atmasvasth.com/speed]
The Book
The Detailed 15-Point Guide to Live Long, Healthy
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.



{kind=link}