Best Case, Worst Case: The Six Questions to Ask Before Surgery
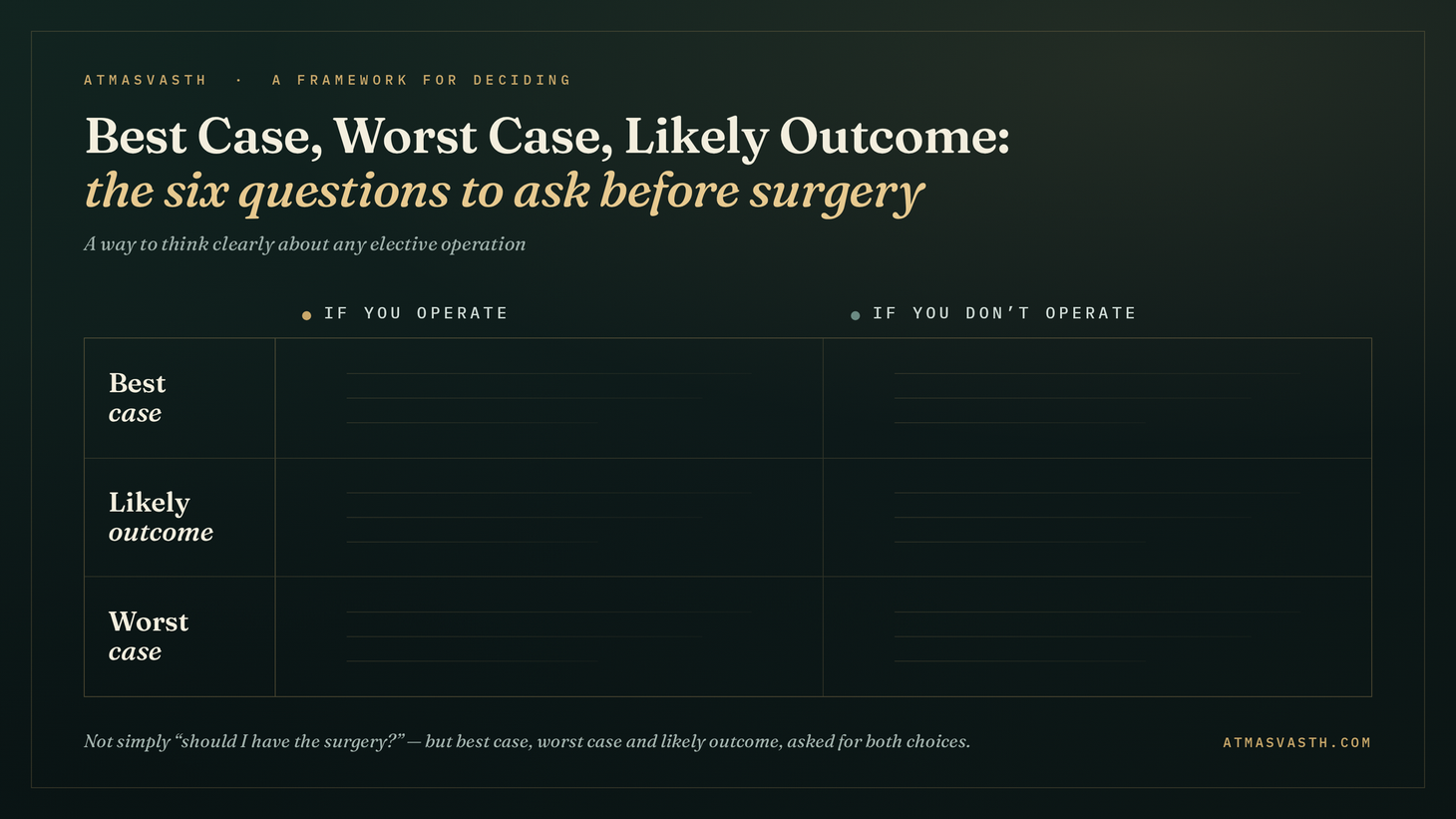
The six question grid helps answer questions about elective surgery
Audio and YouTube versions available at the end of this email.
A reader sent me this query, “my father 74, with ILD (interstitial lung disease), HTN (hypertension), Sugar (diabetes), stroke (reason not known) due to which he had a right eye vision loss and a residual hematoma due to a fall. He has been detected with inguinal hernia, enterocele. I came looking on this blog if there's some article on whether to go for an elective surgery.”
I am not a surgeon, nor a hernia specialist, but when considering elective surgery for a non-emergency situation, there are a few questions they should ask and issues they should discuss with the treating doctor, after being adequately informed.
I am also not a fan of unnecessary surgeries, as I had clearly enunciated in my piece titled “Saying No to Preventive Gallbladder Surgery for Silent Gallstones”, where I argued that just because you are found to have gallstones, there is no reason to get the gallbladder removed.
Is an elective surgery for an asymptomatic hernia the same?
In the gallstone piece, I said, “With any surgery, the dictum has to be, to only let someone operate on you, if it is absolutely necessary. You should be convinced beyond doubt that the surgery will be of help and/or is needed”
So, is an elective surgery for an asymptomatic hernia justified?
It is a good idea to use the scenario setting of best case, worst case and likely outcomes for both operating and not operating based on a framework discussed in detail in the paper by Taylor and colleagues [1] to address this question.
For Operating:
Best case scenario: Patient no longer has a hernia, there is no future risk of strangulation and obstruction and there are no adverse outcomes of surgery and anesthesia.
Worst case scenario: An elective hernia surgery is often a day care procedure, with an extremely low complication rate, even in the elderly. At worst, the patient may land up with chronic groin pain or discomfort that persists beyond the usual recovery period.
Likely outcome: The hernia is no longer evident and there is a slight niggling pain for a month or two at the site of surgery.
For Not Operating:
Best case scenario: Nothing ever happens and the patient will never have a hernia complication and the person goes on living as usual.
Worst case scenario: The hernia gets strangulated and the patient lands up with an acute emergency that may need surgery.
Now, this is where a knowledge of outcomes matters. The INCA study [2] that followed-up patients who opted for watchful waiting vs surgery up to 12 years showed that the rate of strangulation in those who decided to just wait and watch was 3.9%. This means in a room of 100 people with an asymptomatic inguinal hernia who decide to wait and watch, 4 people over 12 years would land up with strangulation.
In short, if asymptomatic, nothing will likely change if you don’t get operated, though there is a 4% chance over 12 years of the hernia getting obstructed.
But this is where things get tricky. While there is usually time to get to a hospital and often the hernia reduces on its own, a surgery for a strangulated hernia will now be a major emergency surgery. A 19,683-patient NSQIP review found elective repair carries similar mortality to the general population while emergency repair is far more dangerous in the elderly [3].
Likely outcome: Nothing will happen for some years, but if the hernia increases, there may be some pain and discomfort.
So to answer the reader’s question.
There is no straight answer.
Surgery for an asymptomatic inguinal hernia is a relatively low-stakes procedure where the chance of complications is quite negligible unlike say a laparoscopic cholecystectomy for asymptomatic gallstones…at the same time, the rate of strangulation is also low enough that watchful waiting will not create a problem in the vast majority of people, though in that small percentage of patients where emergency surgery becomes an issue, the outcomes may be poorer than if it was an elective surgery.

This means that the decision making should be based on a consideration of all personal and related factors including monetary, future life expectancy, etc. It is best to have a frank discussion with the surgeon about best case and worst case scenarios for both operating and not operating and likely outcomes in his/her opinion and then checking with the family physician or cardiologist or geriatrician regarding his general physical and mental condition to go through with the surgery, especially since he has so many other comorbidities as compared to say another 74-years old who is otherwise healthy and fit.
Listening Options
Audio File
YouTube
Footnotes
1. Taylor LJ, Nabozny MJ, Steffens NM, et al. A Framework to Improve Surgeon Communication in High-Stakes Surgical Decisions: Best Case/Worst Case. JAMA Surg. 2017;152(6):531-538.
2. van den Dop LM et al. Twelve-year outcomes of watchful waiting versus surgery of mildly symptomatic or asymptomatic inguinal hernia in men aged 50 years and older: a randomised controlled trial. eClinicalMedicine. 2023.
3. Wu JJ, Baldwin BC, Goldwater E, Counihan TC. Should we perform elective inguinal hernia repair in the elderly? Hernia. 2017 Feb;21(1):51-57. doi: 10.1007/s10029-016-1517-3. Epub 2016 Jul 20. PMID: 27438793.
The Book
The Detailed 15-Point Guide to Live Long, Healthy
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.

{kind=link}