PREVENT over QRisk3 - But Don't Trust a Low Score
Why I'm switching from QRisk3 to PREVENT — and why a low number is a floor, not a clean bill of health.
Audio and YouTube versions available at the end of this email.
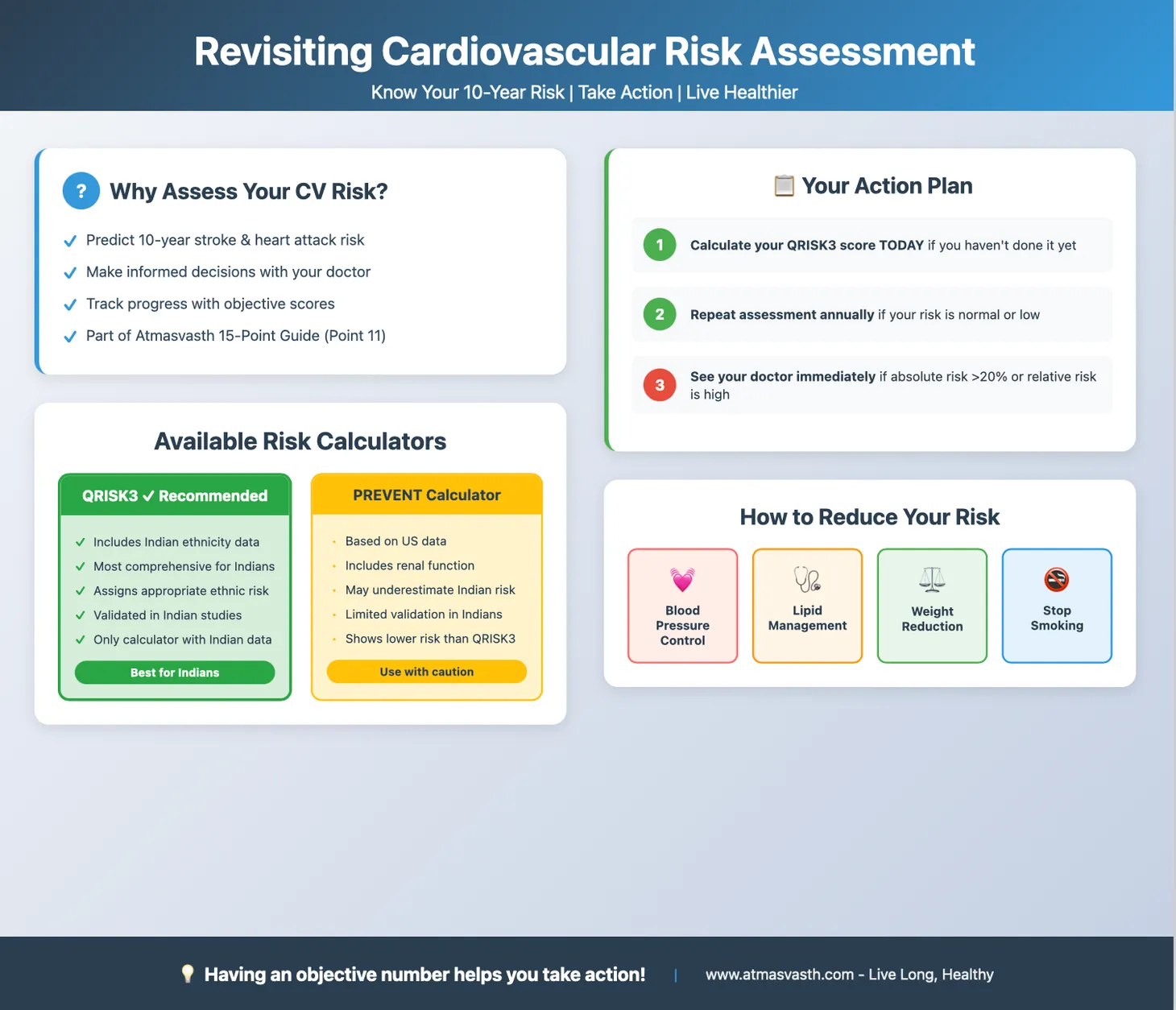
In the 15-point Atmasvasth guide to live long, healthy, the 11th point is "Manage your cardiovascular risk yourself - quarterly, yearly". The 5th subpoint is "Check your QRisk3 score yourself - if the cardiovascular risk is found high, see your doctor. If normal or low, then repeat once a year."
In Aug 2025, I revisited risk assessment mainly because of the growing popularity of the PREVENT calculator and I said that QRisk3 seemed to better identify the so-called extra Indian cardiovascular risk in Indians from India. This was also because QRisk3 did have a small South Asian cohort, though from the UK.
Things have changed in a year.
PREVENT is now the largest validated calculator [1] - 6.4 million people across 62 studies, and it is consistently better calibrated than the older Pooled Cohort Equations (PCEs), though there has been no good head-to-head comparison with QRisk3 and other calculators. PREVENT has also been tested in a South Asian cohort in California [2]…like QRisk3 (South Asians in the UK), these are South Asians in the US, not India, but at least there is now some representation. PREVENT also works beyond the 30-79 age band — in older adults in their 80s [3], and, with weaker evidence, in younger adults too — though the validation is still not absolute.
PREVENT is also the calculator the field has standardised on. The 2025 blood pressure guideline, the 2026 lipid guideline and this week's cardiovascular-kidney-metabolic (CKM) guideline all run on PREVENT [4]. If PREVENT is becoming the common language, then like the one app left standing (Facebook over its competitors, WhatsApp over its rivals), it will likely become the de facto equation used around the world. One caveat though - wider use makes it the standard, but a calculator gets better at estimating risk only when it is recalibrated on fresh data, not simply by being used more.
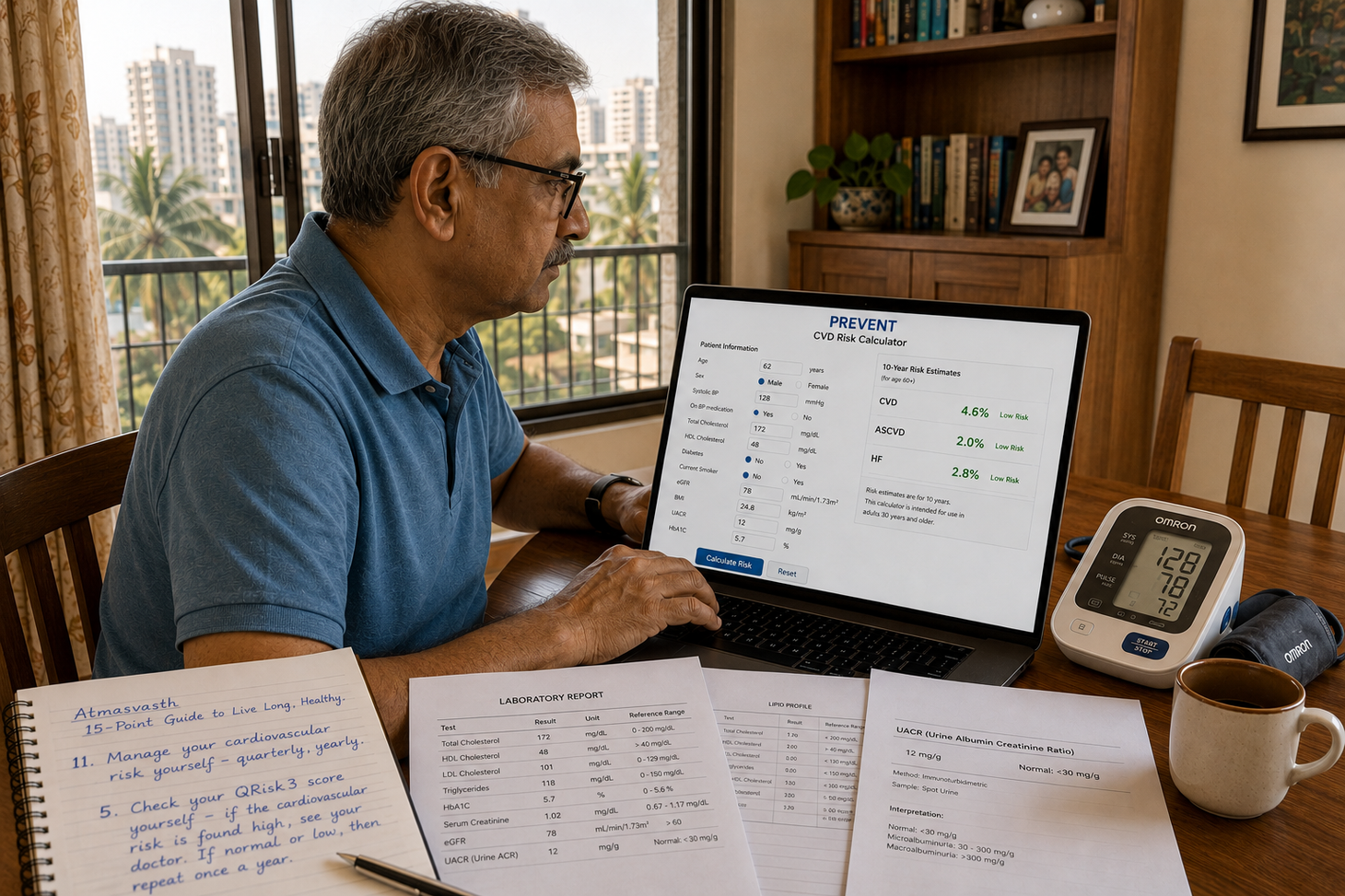
It is easy to use the PREVENT calculator. It needs your age, sex, systolic blood pressure, whether you take blood-pressure-lowering medication, total cholesterol, HDL cholesterol, diabetes status, current smoking status, eGFR, BMI, urinary albumin (UACR) and HbA1C. It will give you 10 and 30 year risk estimates if you are 59 or under and just 10 year risk estimates if you are 60 or older. There are 3 risks calculated, CVD (total cardiovascular disease), ASCVD (atherosclerotic cardiovascular disease) and HF (heart failure).
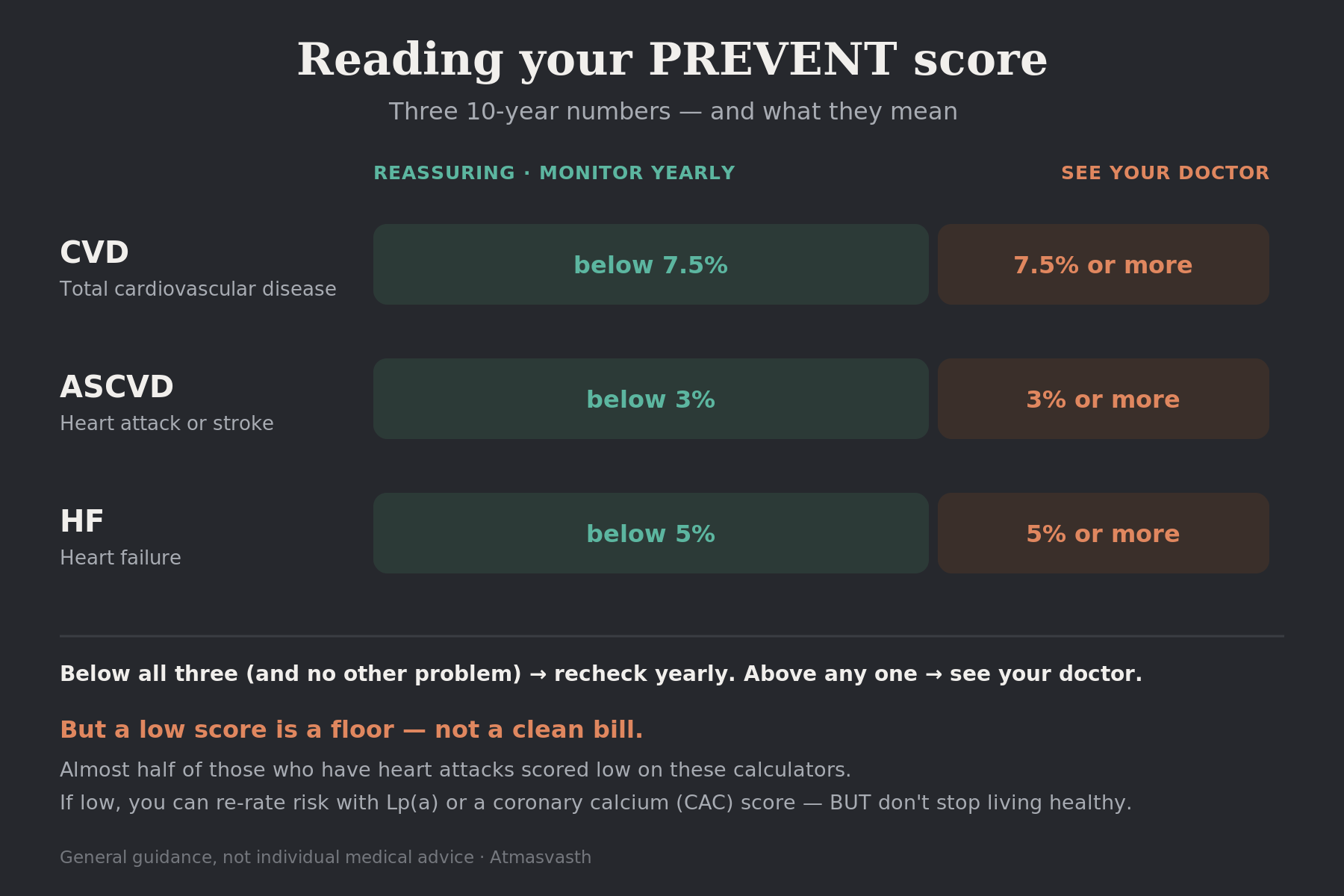
Depending on your underlying medical situation, the risk estimates will help you understand what to do next. Typically if the 10-year CVD risk is <7.5%, the ASCVD risk < 3% and the HF risk < 5% and you have no other disease, you need not see a doctor for risk assessment.
Just to clarify what these percentages mean. A CVD risk of 10% means that in a room of 100 people with the same risk profile as you, 10 people are likely to get an event (heart attack, stroke, heart failure) over 10 years. An ASCVD risk of 10% means that in a room of 100 people with the same risk profile as you, 10 people are likely to get either a heart attack or stroke or both over 10 years. A HF risk of 10% is similar, but for heart failure alone.
In younger people, a 30-year risk estimate is also calculated, but this has to be titrated against the age-expected risk in the form of percentiles. This website has charts to help estimate these percentiles [5] (it runs on a free server, so it may be intermittently available).
The calculators are not infallible, typically in younger people, specifically in India, specifically with 10-year risk estimates, as a study from Jabalpur showed [6] where those under 40 with heart attacks had 10-year risk estimates of 1.5% but 30-year risk estimates that were more realistic. Another study from North India headed by Mohit Gupta [7] showed that in over 6000 first time STEMI heart attacks (the bad kind of heart attacks), one in four had no standard modifiable risk factor such as high blood pressure, diabetes, abnormal lipids or smoking. This was also true of a US based study in 2025 where 61% of those who presented with a heart attack had low or borderline PREVENT scores [8].
So what does this mean for you and me?
First, get the blood tests needed for inputting into the PREVENT calculator. Then use the calculator.
If you are above 60 and the risk is low, nothing much needs to be done, as long as you have no other disease or problem that needs addressing…you just need to check the risk every year. However, since low risk is not zero risk since almost half of those with heart attacks often have low risk on these calculators, you could also look at newer parameters such as lipoprotein(a), which I wrote about in Jun 2025, or calcium score on CT, both of which may rerate the risk.
Philosophically and practically though, there are only so many tests you can do before you run into a wall of diminishing returns. And...even if you score a low risk on these calculators, you cannot stop doing everything possible to live long, healthy…from moving, to eating sensibly to sleeping well, etc...these are non-negotiable.
If the risk is high, then it matters. Please see your doctor to figure out how to reduce that risk. If you are younger and the 10-year risk estimate is low, but the 30-year estimate is high, check the percentiles and see your doctor to understand if anything needs to be done…if not, then just monitor the risk every year using the same parameters.
Listening Options
Audio File
YouTube
Footnotes
- Neuen BL, Major RW, Grams ME, et al. Multinational validation of the PREVENT and SCORE2 cardiovascular risk equations across 6.4 million individuals. Nat Med. 2026. doi:10.1038/s41591-026-04437-z.
- Yan S, Gupta S, Go AS, et al. Performance of the American Heart Association's PREVENT Equations Among Disaggregated Racial and Ethnic Subgroups. JAMA Cardiol. 2025;10(9):876–885. doi:10.1001/jamacardio.2025.1865.
- Fravel MA, et al. Performance of the American Heart Association PREVENT Cardiovascular Risk Equations in Older Adults. Circ Cardiovasc Qual Outcomes. 2025. doi:10.1161/CIRCOUTCOMES.124.011719. (PMID 40289804.)
- Khan SS, Bhave N, Blumenthal RS, et al. Use of Predicted Risk and Expected Benefit to Guide Decision-Making in Cardiovascular-Kidney-Metabolic Syndrome: A Scientific Statement From the American Heart Association and American College of Cardiology. Circulation. 2026;153. doi:10.1161/CIR.0000000000001447. (The CKM guideline itself: Ndumele CE, et al. 2026 AHA/ACC/ADA/ASN Guideline for the Prevention, Detection, Evaluation, and Management of Cardiovascular-Kidney-Metabolic Syndrome. Circulation. 2026;153. doi:10.1161/CIR.0000000000001453.)
- Krishnan V, et al. Age- and Sex-Specific Percentiles of 30-Year Cardiovascular Disease Risk Based on the PREVENT Equations. J Am Coll Cardiol. 2025. doi:10.1016/j.jacc.2025.09.1509.
- Jharia A, et al. Can QRISK-3 and PREVENT Predict Premature Acute Coronary Syndrome? The PRACS-40 Study. Heart Views. 2025. doi:10.4103/heartviews.heartviews_171_25.
- Gupta MD, Raturi P, Palleda GM, et al. Clinical Profile and Outcomes of ST-Segment Elevation Myocardial Infarction Without Standard Modifiable Risk Factors. JACC Asia. 2026;6(2). doi:10.1016/j.jacasi.2025.10.005.
- Mueller AS, Leipsic J, Tomey M, Argulian E, Narula J, Ahmadi A. Limitations of Risk- and Symptom-Based Screening in Predicting First Myocardial Infarction. JACC Adv. 2025;4(12):102361. doi:10.1016/j.jacadv.2025.102361.
Atmasvasth Shop
The Detailed 15-Point Guide to Live Long, Healthy
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.

{kind=link}