Should You Take Ozempic or Mounjaro if You are Not Obese or Diabetic?
There is no data to support the use of GLP-1 and GIP receptor agonists like Ozempic and Mounjaro if you are not obese or diabetic, but people are using them anyway...this becomes an individual personal call and there is no right or wrong here.
The Book - Kindle Version Now Available Worldwide
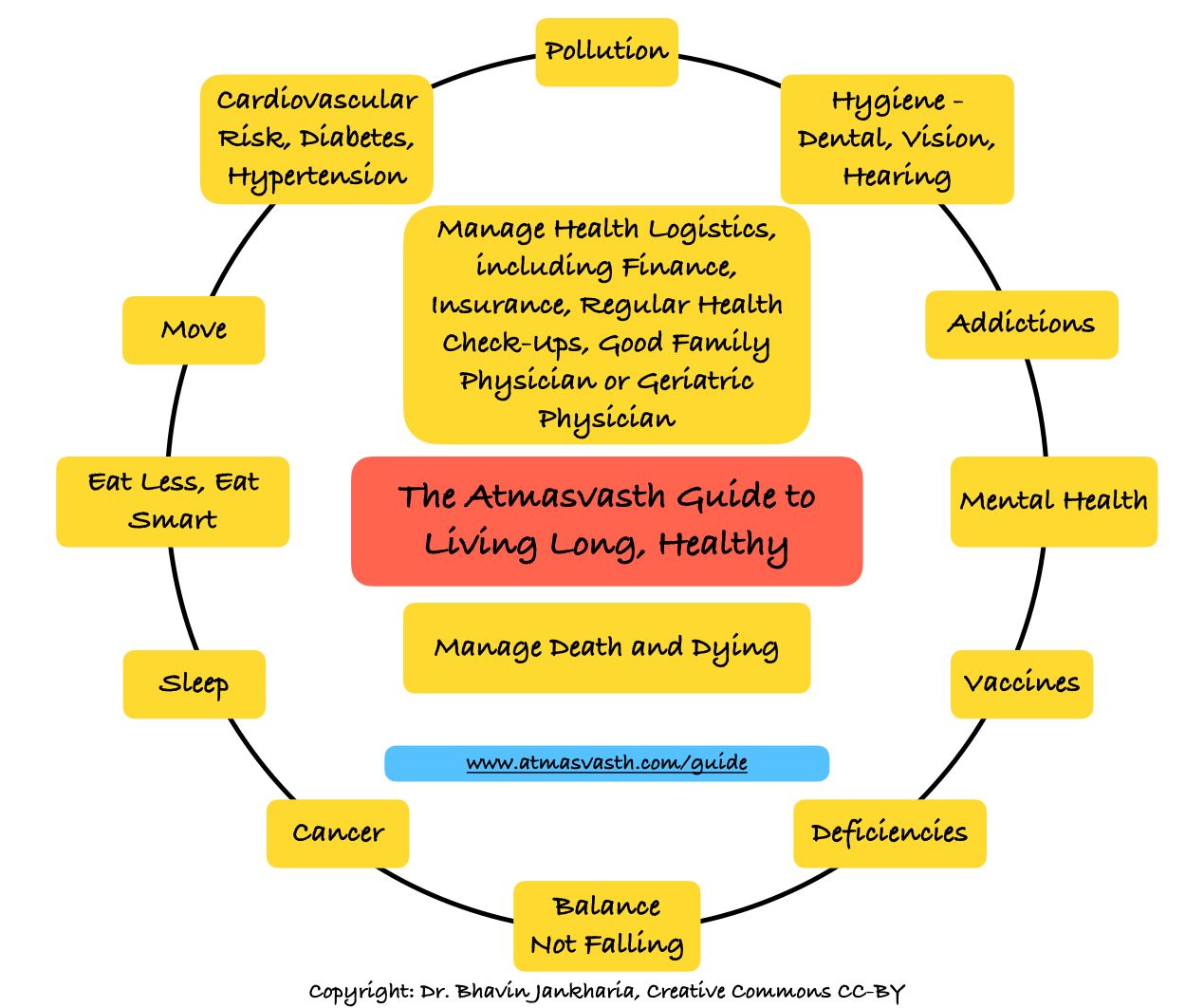
The Detailed 15-Point Guide to Live Long, Healthy
Audio
Soundcloud
YouTube
A YouTube version of the audio is also now available here.
Text
Last fortnight, I introduced the concept of a GLP-1 receptor agonist drug semaglutide, in the context of its ability to reduce hepatic steatosis and fibrosis, which is a game-changer, because there was no real treatment available for this common condition that can potentially lead to liver failure.
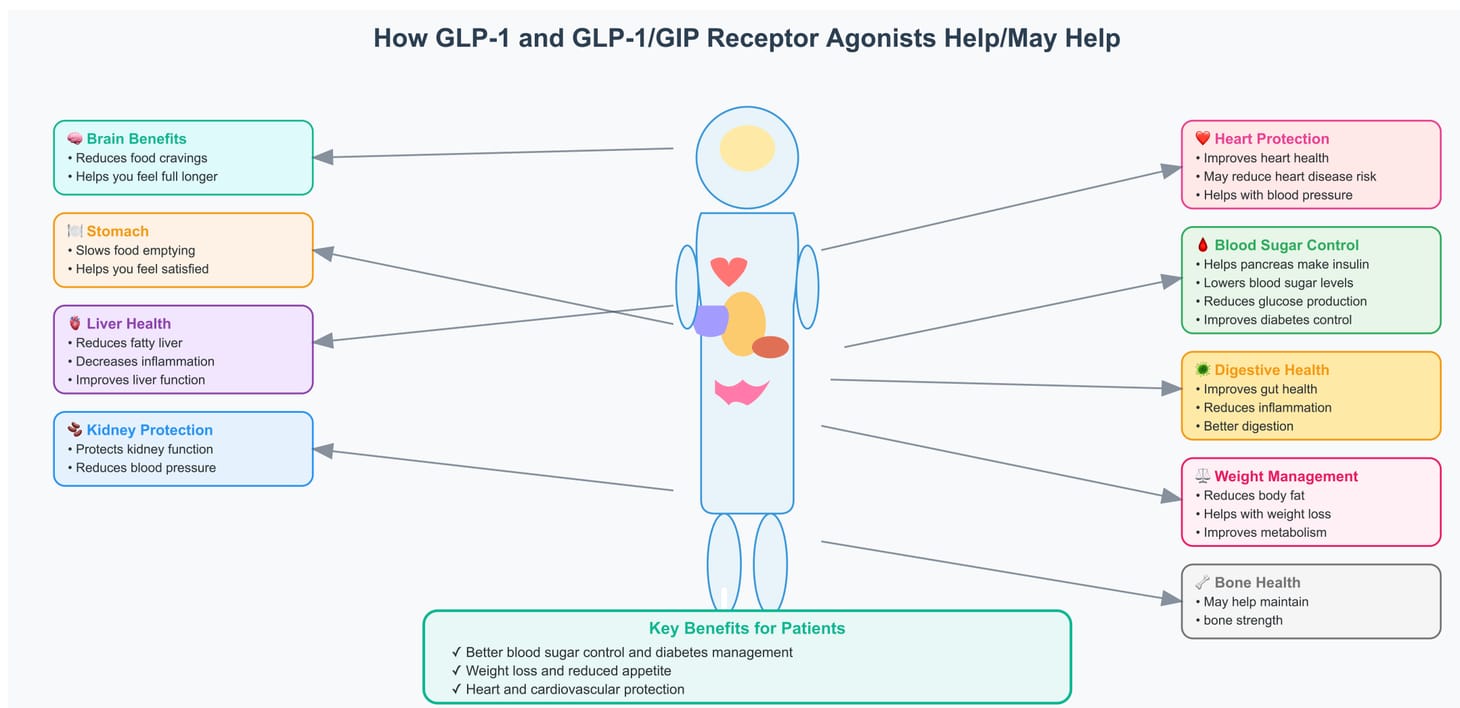
Many of you must have come across news reports of these new apparently wonder drugs (Ozempic, Mounjaro) that help people with diabetes [1] and obesity [2]. These are GLP-1 (glucagon-like peptide-1) receptor agonists, a class of incretin hormone agonists, working primarily by mimicking the action of GLP-1, which triggers the pancreas to release more insulin and by increasing satiety at multiple levels, to reduce appetite, hunger and hence, food intake. One sub-class is the GLP-1/(glucose-dependent insulinotropic polypeptide) GIP receptor agonist (tirzepatide) that also targets GIP receptors apart from GLP-1 receptors.
Tirzepatide (Mounjaro) is currently the only such injectable available in India, while semaglutide (injectable Ozempic) is only available in its oral form, which is not the standard method of use.
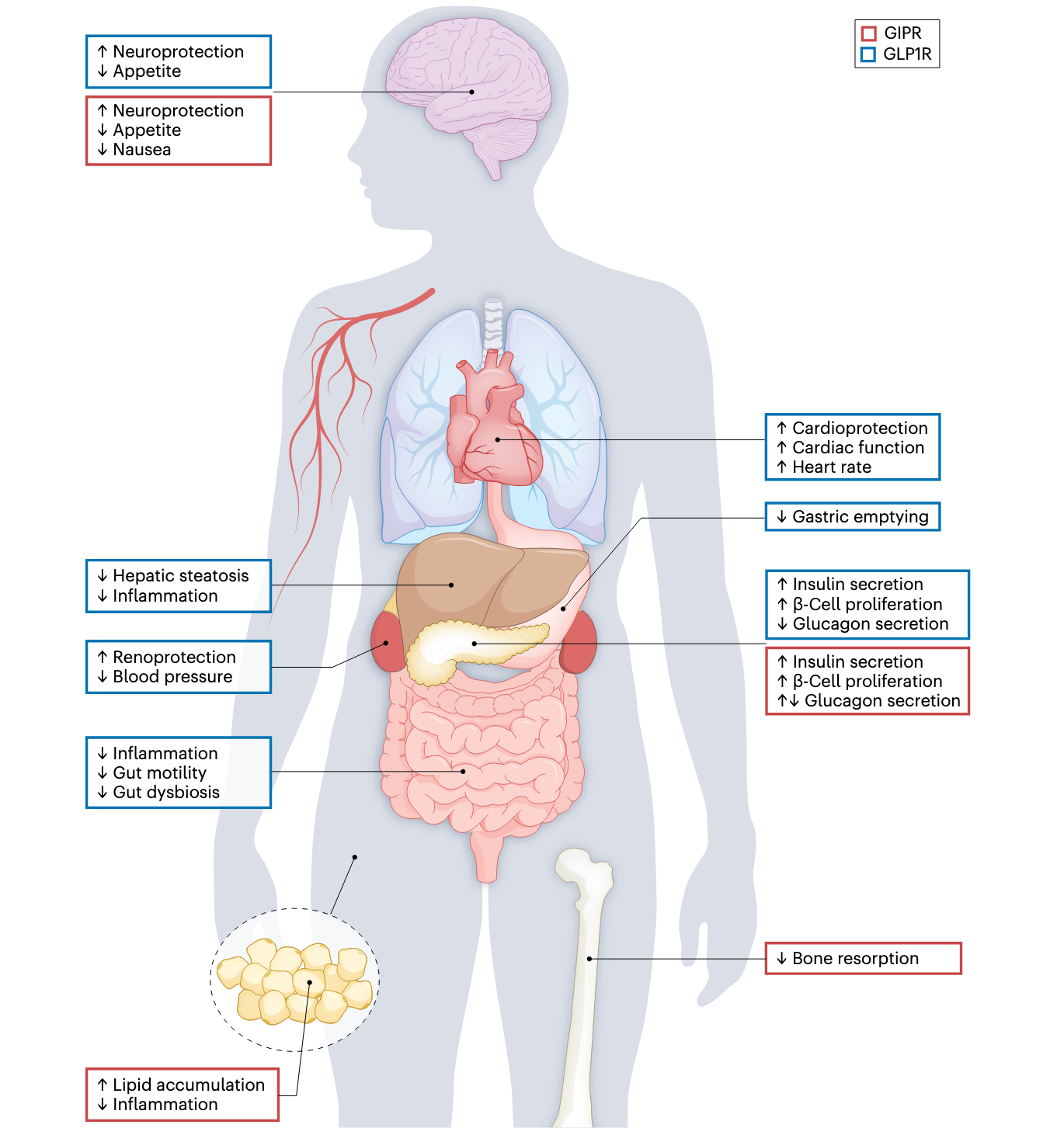
GLP-1 receptors are present not just in the pancreas, but also in the brain, cardiovascular and immune systems, gut and kidney, thus also causing extrapancreatic actions. Here is a diagram showing the potential uses and actions [3] taken from an article by Hammoud and colleagues.
Currently good, hard data is only available for their use in reducing weight and controlling blood sugar in patients with obesity and diabetes respectively, along with improved outcomes of adverse events and all-cause mortality. There is also data slowly accumulating on other benefits, e.g. improved cardiovascular protection in those who are obese [4] or diabetic, reduced pain from knee osteoarthritis (the commonest cause of knee replacement) in obese patients [5] and reduced hepatic fat and fibrosis, the mechanism of action in all of them being over and above that which would be attributable only to weight loss and blood sugar control.
Observational studies have shown improvement of blood pressure, delayed cognition loss and reduced pain and inflammation, perhaps protection against some obesity-related tumors and improving sleep in those with obstructive sleep apnea.
Why this article? One of my readers emailed me saying that with so much evidence of off-label use, why are doctors not promoting the use of these drugs for all of these conditions, outside of obesity and diabetes. This is also likely spurred by the use of these drugs by celebrities to look lean (you can make out they are using GLP-1 agonists by looking at their faces, which show a typical contouring with prominent cheekbones and exaggerated wrinkles (The Ozempic Face), which many of our Indian celebrities seem to have as you can see in these two YouTube videos [6], [7]. These drugs have entered regular conversations and there are many reports of people using them prior to weddings or events to lose weight and to look good, if not permanently then temporarily.
Some of this hype feels like that of vitamin D, which is supposed to be the one-cure all for almost every disease in the world, but hasn’t been proven to be of any use, unless you are deficient.
GLP-1 receptor agonists are different because there is good data from so many RCTs conducted by so many different groups of researchers and replicated by other subsequent trials. They are game changers, because they are likely to reduce the need for bariatric surgery, liver transplants and knee replacements among other possible seismic changes.
The drugs are not without side effects that include nausea, vomiting and diarrhea, rarely pancreatitis and some forms of rare cancers in patients who have a family history of such cancers. The other challenge is that when they are stopped, most of the changes including weight loss, reverse.
What does this mean for you and I?
If you are obese and if you are not fit (it is better to be fit and overweight rather than thin and unfit), and if nothing is working, or if you are diabetic and taking drugs (metformin, insulin) anyway, or have both, there is clear data that you should start Ozempic or Mounjaro with the help of your doctor, who may or may not be up to date with the use of these drugs. If you have pain due to knee degeneration, you may want to try these before going in for knee replacement. If you have hepatic steatosis, these drugs will help.
But what if you are not obese, or just a bit overweight or normal weight and not diabetic and do not have hepatic steatosis or knee degeneration? Should you take these drugs to lose just a couple of kilos or perhaps keep your blood pressure better controlled? There is no data currently to suggest you should, but people are taking them anyway. You may have also heard of microdosing because of influencers or articles, but again there is no data to support their use.
If you are being seduced into trying them, that is an informed decision you have to take based on all the information I have presented here and your own reading and understanding of your health and life. There is no right or wrong here...if you believe they will help you, go ahead but if you want to wait for more data, that is fine, too.
Two articles, one in The Atlantic and one in the New York Times, both written by the same person, David Kessler, who was a former commissioner of the US FDA, may also help. He argues that in a world where it is difficult to control what we eat, and that a lot of what we eat is ultra-processed or more importantly, ultra-engineered to make us want more, using drugs to control our appetite and weight may be acceptable, short term or long term.
I will keep adding to this information in the years to come, because these drugs are here to stay and it is highly possible that they may be of help in our atmasvasth quest to live long, healthy.
Footnotes
1. Frías JP et al. Tirzepatide versus Semaglutide Once Weekly in Patients with Type 2 Diabetes. N Engl J Med. 2021 Aug 5;385(6):503–15.
2. Rubino D et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021 Apr 13;325(14):1414.
3. Hammoud R, Drucker DJ. Beyond the pancreas: contrasting cardiometabolic actions of GIP and GLP1. Nat Rev Endocrinol. 2023 Apr;19(4):201–16.
4. Lincoff AM et al. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023 Dec 14;389(24):2221–32.
5. Bliddal H et al. Once-Weekly Semaglutide in Persons with Obesity and Knee Osteoarthritis. N Engl J Med. 2024 Oct 31;391(17):1573–83.
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.

{kind=link}