A Simple Polypill to Change Lives
A polypill with one anti-hypertensive drug and one statin has the power to dramatically reduce cardiovascular risk and events in those around us at an extremely affordable, low cost.
The Book
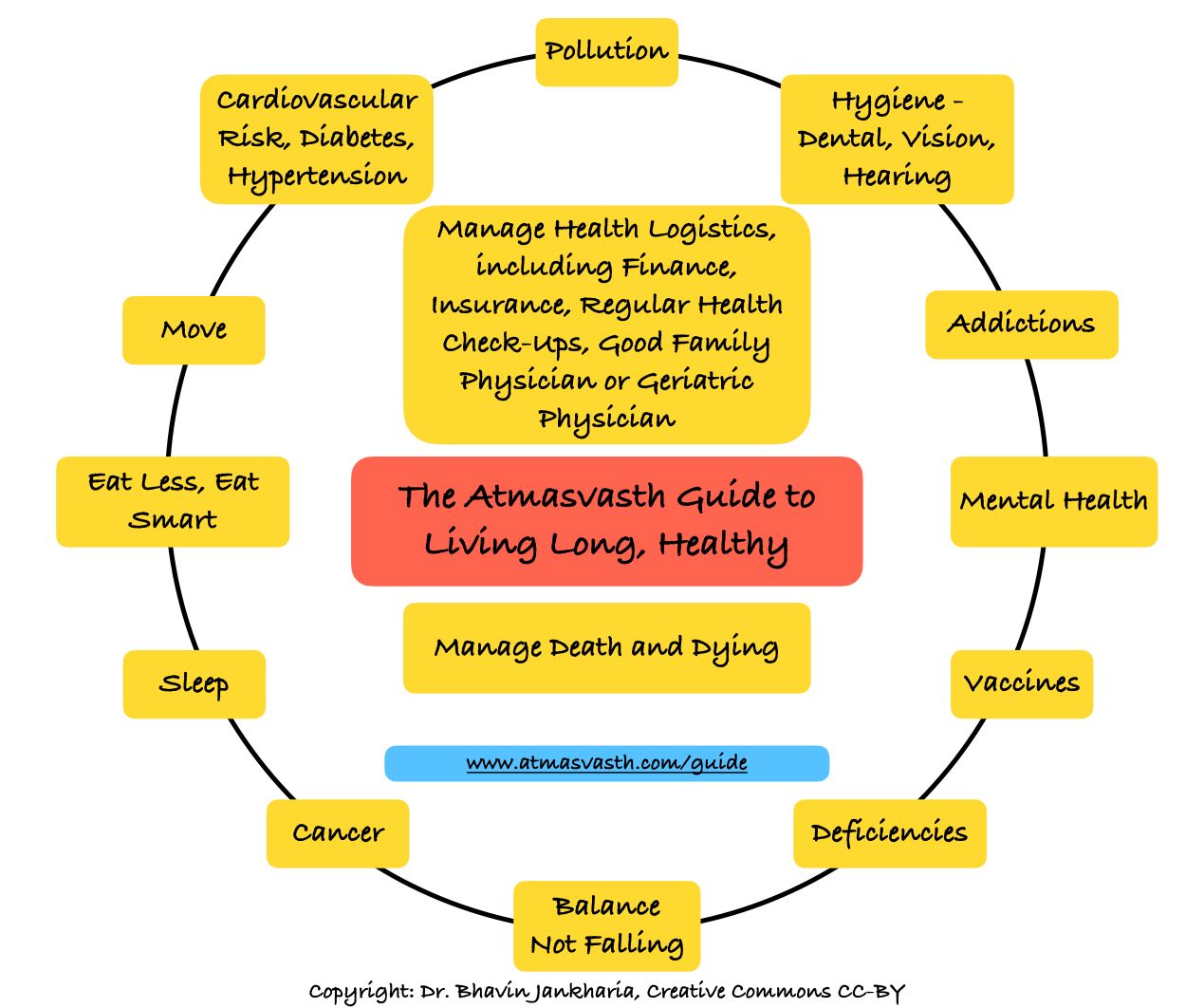
The Detailed 15-Point Guide to Live Long, Healthy
Audio
Soundcloud
YouTube
A YouTube version of the audio is also now available here.
Text
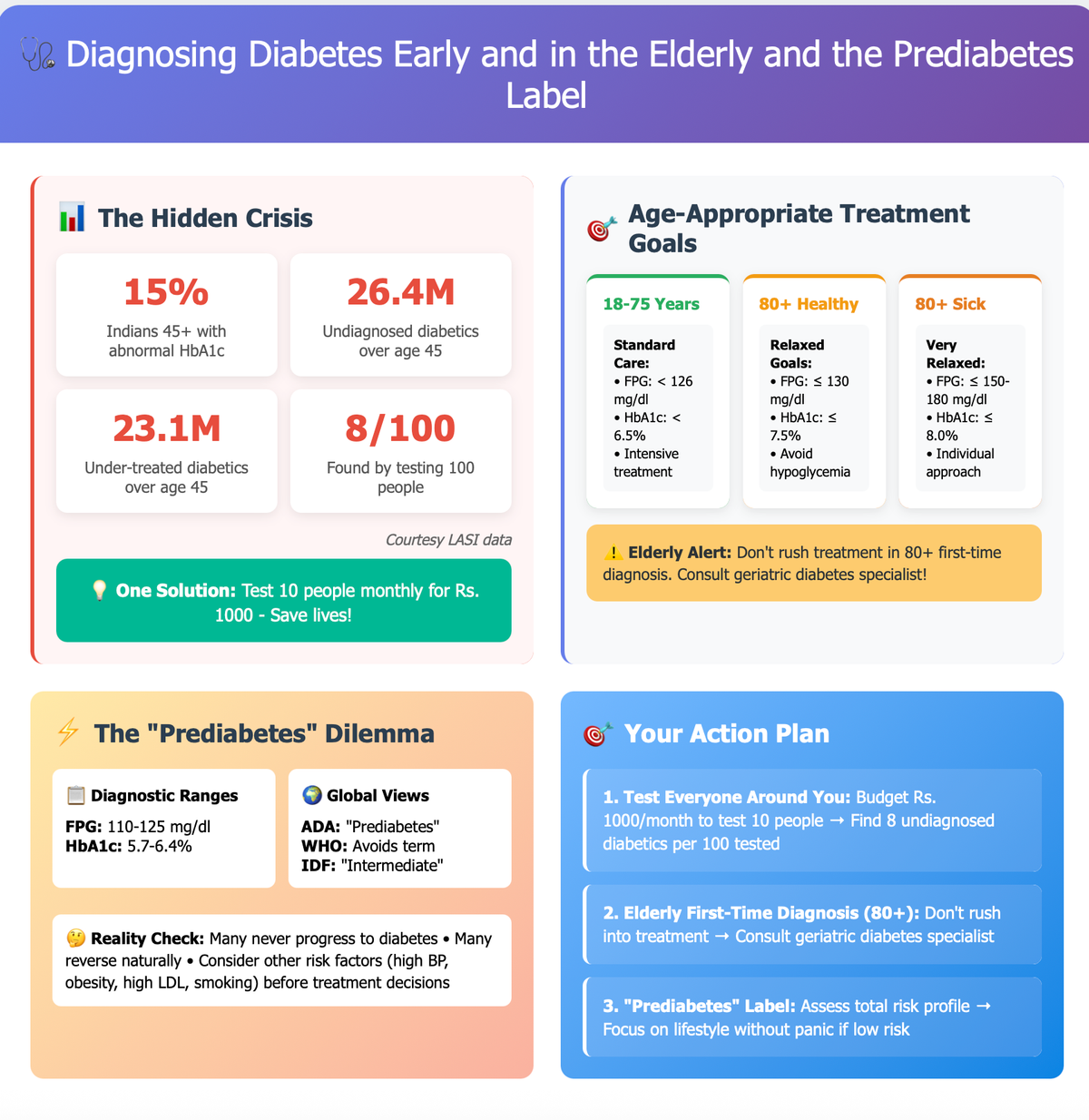
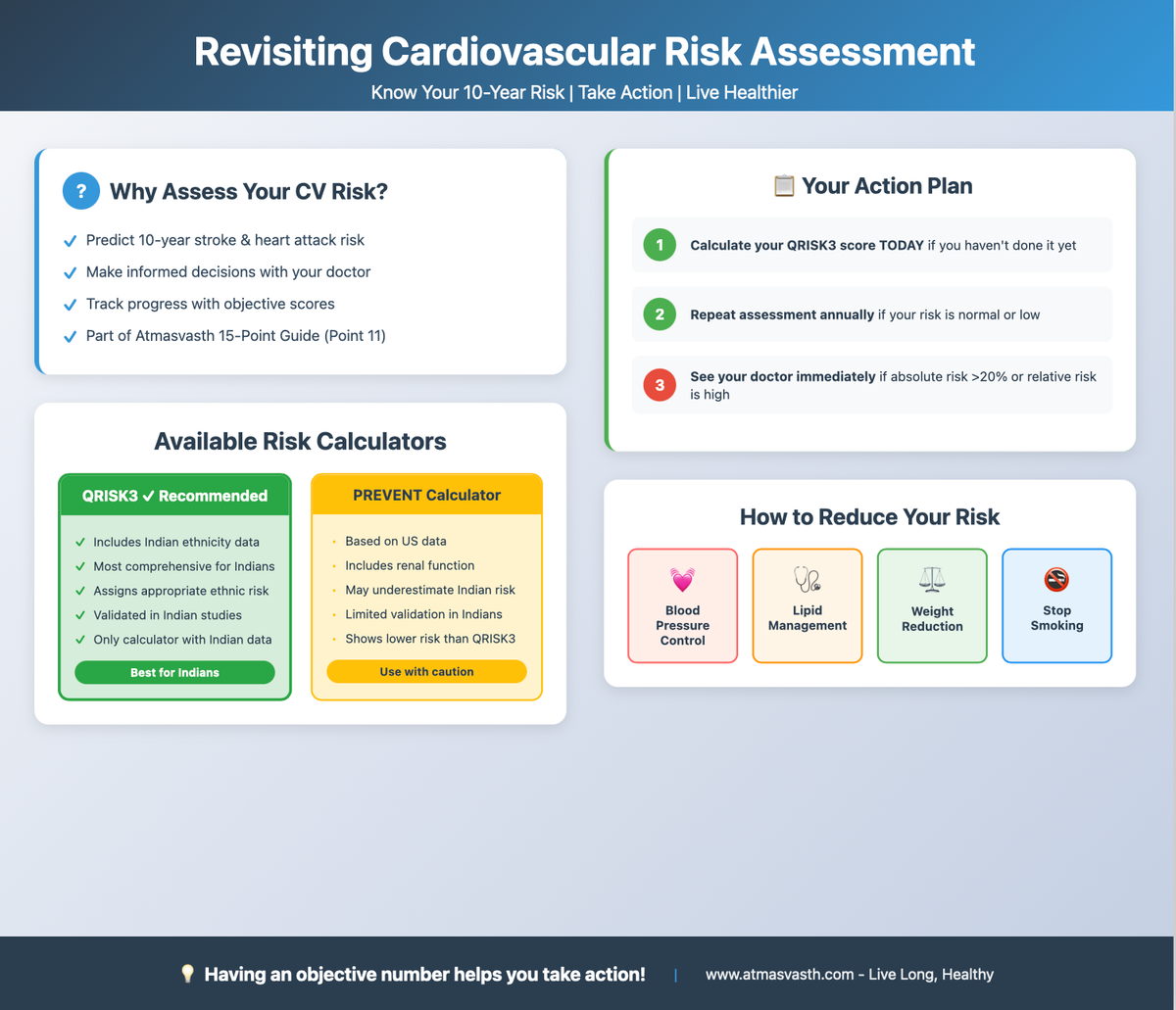
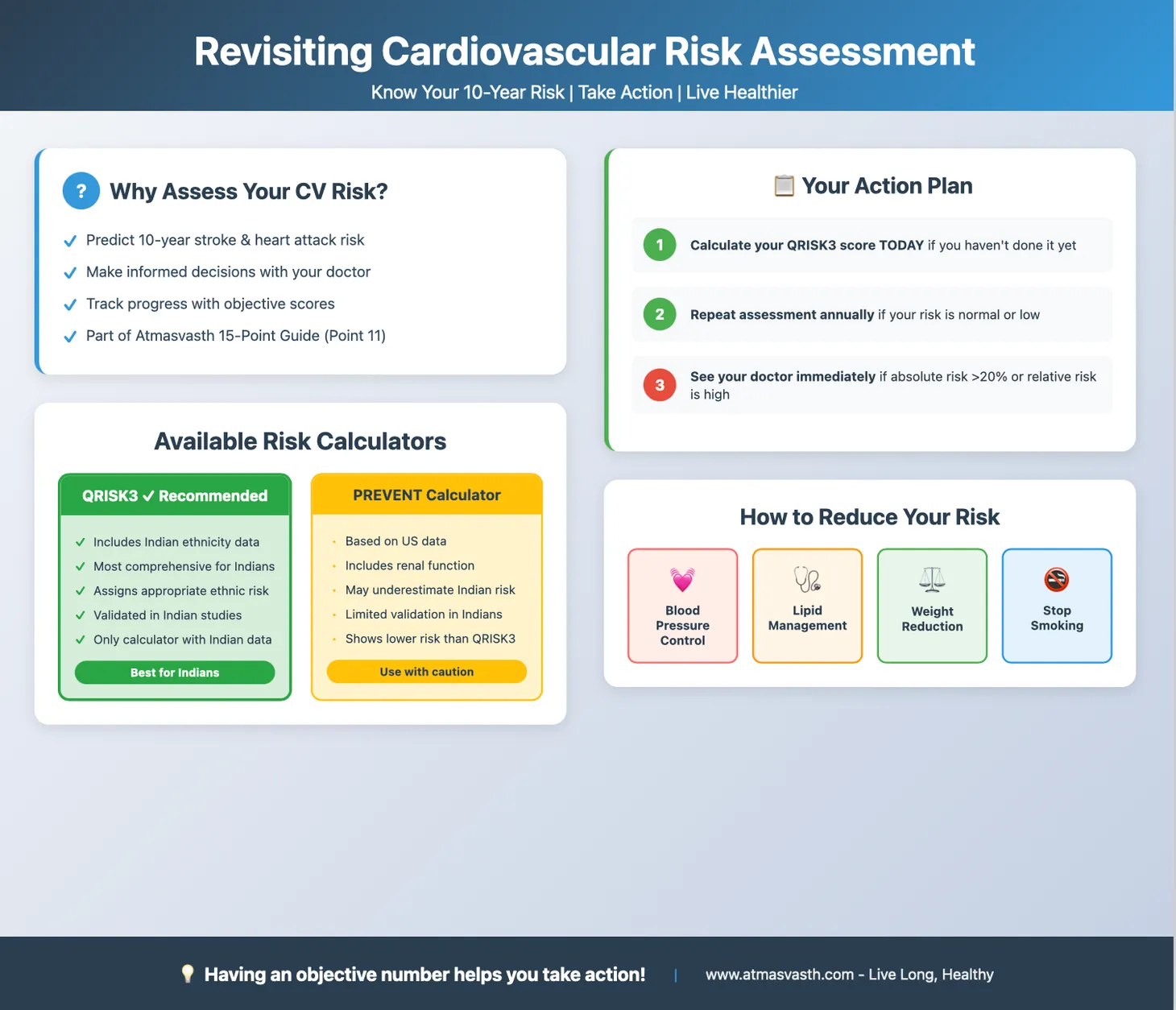
In Jul 2025, I discussed the “cardiovascular syndemic”, the 5 threats of high blood pressure, high blood sugar, high lipid levels, obesity and smoking and then followed it up with a piece on diagnosing diabetes early and then an article on revisiting risk assessment and QRISK3.
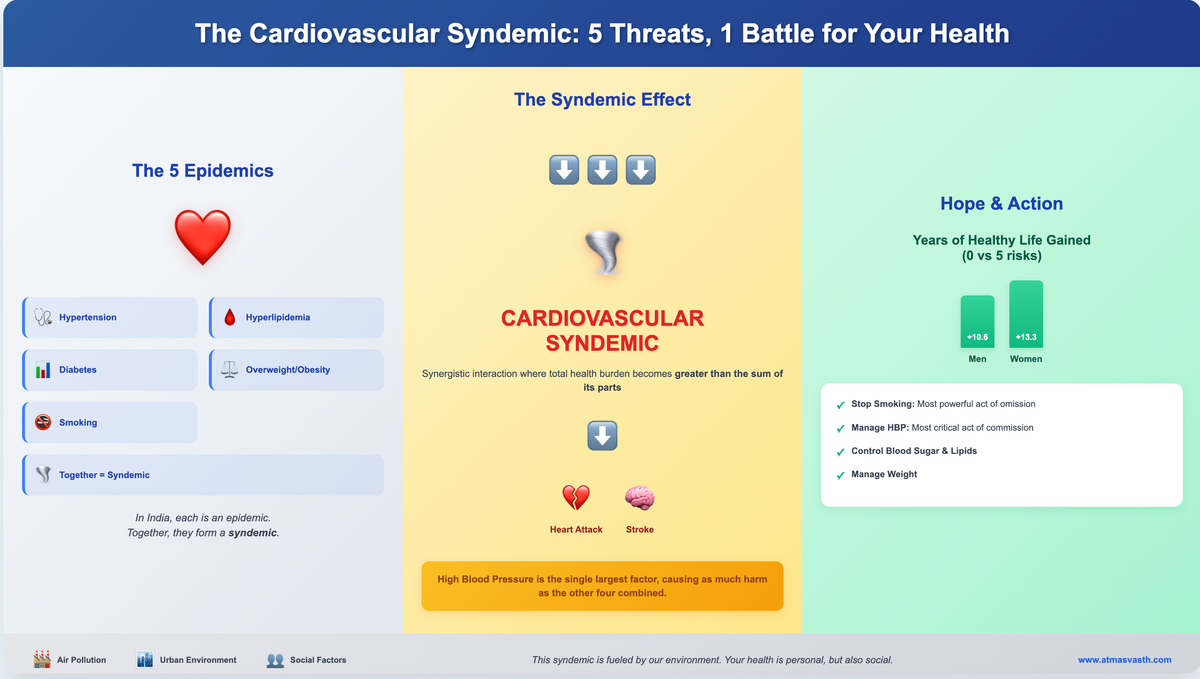
I am focusing on cardiovascular risk over others such as cancer risk, mainly because heart attacks, heart failure and strokes are far commoner causes of disability and death than cancers. Cancer care however is glamorous and so even the public health focus is on building more cancer hospitals, rather than detecting and controlling high blood pressure, the single biggest killer in our country and the world and high blood sugar, which is among the top 5 killers.
This often leads to situations where people have cardiovascular events like stroke, heart attacks and heart failure and we hear the common refrain…but there was nothing wrong, it’s been all sudden…perhaps it was the stress of living in Mumbai that caused this.
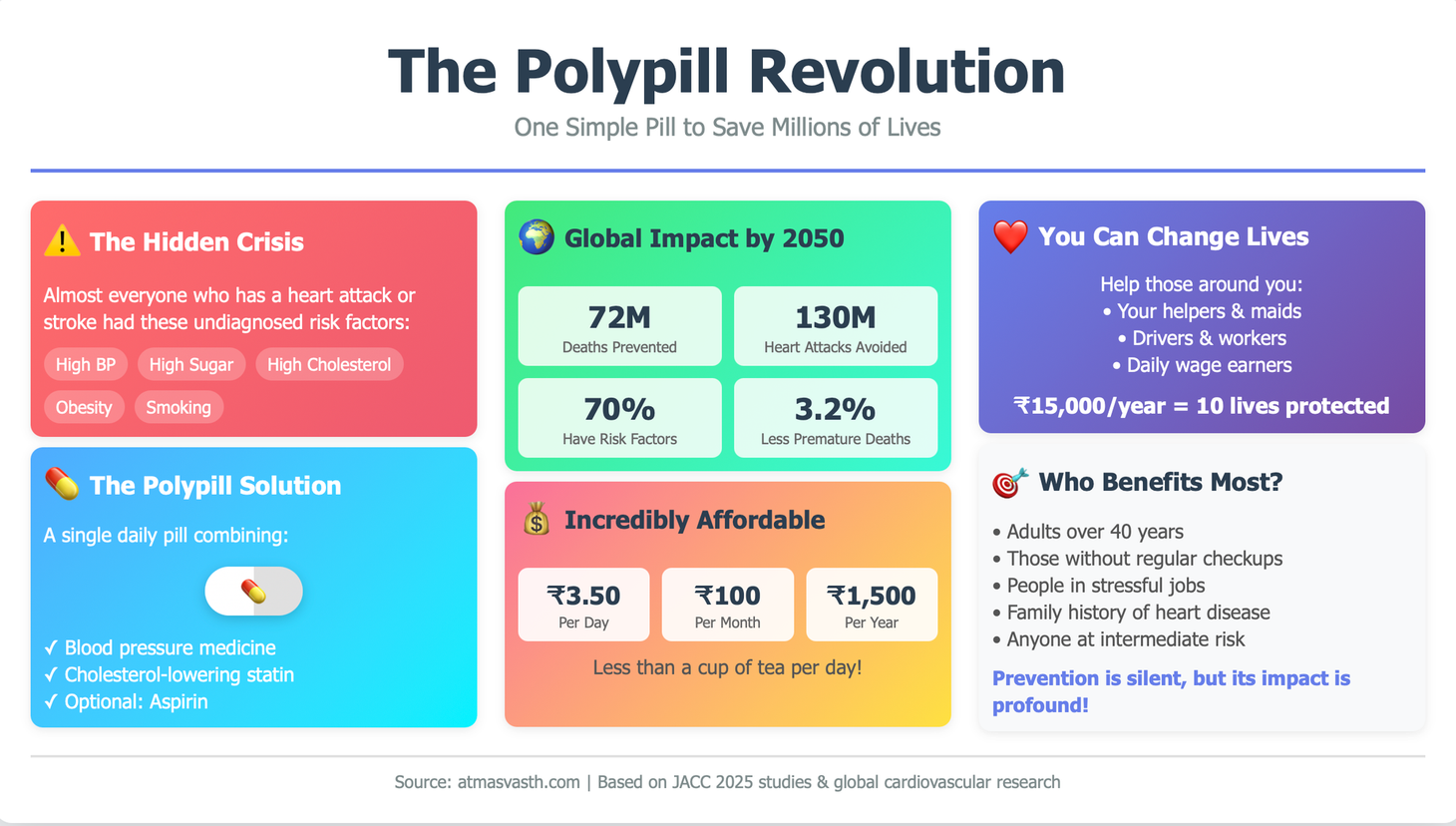
A recent paper exposes that “lie”. The authors led by Hokyou Lee [1] analyzed two public cohorts, in South Korea and the US and found that in virtually every patient who had a cardiovascular event, there was always a non-optimal risk factor present (non-optimal blood pressure, blood sugar, cholesterol, or the patient was a smoker). This means that the prevalence of undiagnosed non-optimal risk factors in the population is high and when uncorrected or undiagnosed can lead to an event that reduces healthspan and lifespan. Conversely, identifying and correcting these risk factors, can potentially reduce the risk of CV events or eliminate their occurrence, thus increasing healthspan and lifespan.
With this in mind, there was an experiment carried out during cricket matches by a foundation started in the name of Shane Warne. Pop-up health check up stations were installed at events (mainly cricket events) and at pharmacies and they found that almost 70% of patients had one uncontrolled risk factor [2]…and this is Australia, a health-conscious nation. If such stations were installed in India, the number of people across all socio-economic strata who would be found to have one or more risk factors, would probably be much higher.
If the burden of cardiovascular disease is so high, and if a large number of people, despite being educated remain undiagnosed, perhaps another simpler solution is needed.
One such method is to eliminate the need to test for high blood pressure and high cholesterol and to dispense a polypill (a single pill combination) consisting of one statin and one or more antihypertensive drugs, with or without aspirin to adults.
A recent modeling study [3] has suggested that a polypill strategy could prevent up to 72 million deaths and 130 million cases of stroke and heart diseases, in those at intermediate to high risk, especially in South and South-East Asia and reduce all-cause premature mortality by 3.2% over 2023-2050. This was based on earlier randomized controlled trials that have shown significant effectiveness of polypills in the general population.
A study looked at affordability [4] and found that a combination of aspirin, atorvastatin and ramipril would cost 1.26 USD or approx. Rs.100 per month or Rs. 3.50 per day in India. This is affordable and has the potential to significantly change lives by reducing cardiovascular morbidity and mortality. A polypill without aspirin, especially if being used in the general population without risk assessment would come at a further reduced cost. A quick check today shows a price point between Rs. 3.9 to Rs. 4.5 per tablet/capsule, which can be brought down further with bulk orders.
Are there downsides of giving a blood-pressure lowering drug and a lipid lowering drug together to the general population without testing? In otherwise healthy individuals, there are none. Statin-related myopathy may occur and if people complain about muscle pains, then this could be addressed, but the risk of complications is extremely low, especially when aspirin is omitted.
It could be argued that this is a patronizing, paternalistic approach. But in a setting, where the vast majority of people remain undiagnosed, perhaps this is a way to reduce morbidity and mortality.
What would a typical scenario? A polypill could be dispensed to everyone around us - our maids, helpers, house-helps, drivers, workers, those who come home for different errands, the garbage collectors…people around us who make our lives better. If each of us wanted to do this, it would cost around Rs. 1500 per person per year to change a life. If we decided to change 10 lives, that would be Rs. 15,000 per year.
This does not include an anti-diabetic medicine, but those who agree to take the polypill would also by and large agree to a fasting blood sugar test that would cost Rs. 30-100 and if the FBS is found to be high, we could help them with a metformin tablet at Rs. 1.2 per tablet, which would perhaps bring the combination to Rs. 5 per person per day. The reason we can’t randomly add an anti-diabetic drug to the polypill is because of the real chance of hypoglycemia (while hypotension - reduced blood pressure is not an issue) and hence the need to test and titrate diabetic medications.
I have been thinking about this for a while and am planning to start enrolling those around me into a polypill program. The challenge will always be that those who benefit won’t fall sick and won’t appreciate the benefit, but that is the whole point of prevention anyway, isn’t it? If they do continue to take a polypill + antidiabetic (if necessary) for life, perhaps that will have a significant impact, at a price that many of us can afford to help those around us.
Footnotes
1. Lee H, Huang X, Khan SS, Son D, Lee HH, Kim EJ, et al. Very High Prevalence of Nonoptimally Controlled Traditional Risk Factors at the Onset of Cardiovascular Disease. JACC. 2025 Oct;86(14):1017–29.
2. Tan S, Nelson AJ, Muthalaly RG, Nerlekar N, Duncan N, Nolan HP, et al. Pop-Up Cardiovascular Screening Within Community Pharmacies and an International Sporting Event. JACC. 2025 Sept;86(13):950–8.
3. Watkins DA, Pickersgill SJ, Flood D, Gaziano TA, Huffman MD, Islam S, et al. Global Impact of Fixed-Dose Combination Therapies on Cardiovascular Mortality and Events, 2023-2050. Journal of the American College of Cardiology. 2025 July;86(3):149–61.
4. Satheesh G, Gyawali B, Sun MFC, Huffman MD, Banerjee A, Perel P, et al. A Survey of Availability and Affordability of Polypills for Cardiovascular Disease in Selected Countries. Global Heart [Internet]. 2024 July 1 [cited 2025 July 20];19(1). Available from: https://globalheartjournal.com/articles/10.5334/gh.1335/
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.


{kind=link}