Sarcopenia, Muscle Failure, Dynapenia - Understanding, Preventing and Managing
Sarcopenia is of growing concern in the elderly. It is preventable if we act now in our 60s. However, in those older around us, we should learn to recognize and then treat or manage.
The Book
The Detailed 15-Point Guide to Live Long, Healthy
Audio
Soundcloud
YouTube
A YouTube version of the audio is also now available here.
Text
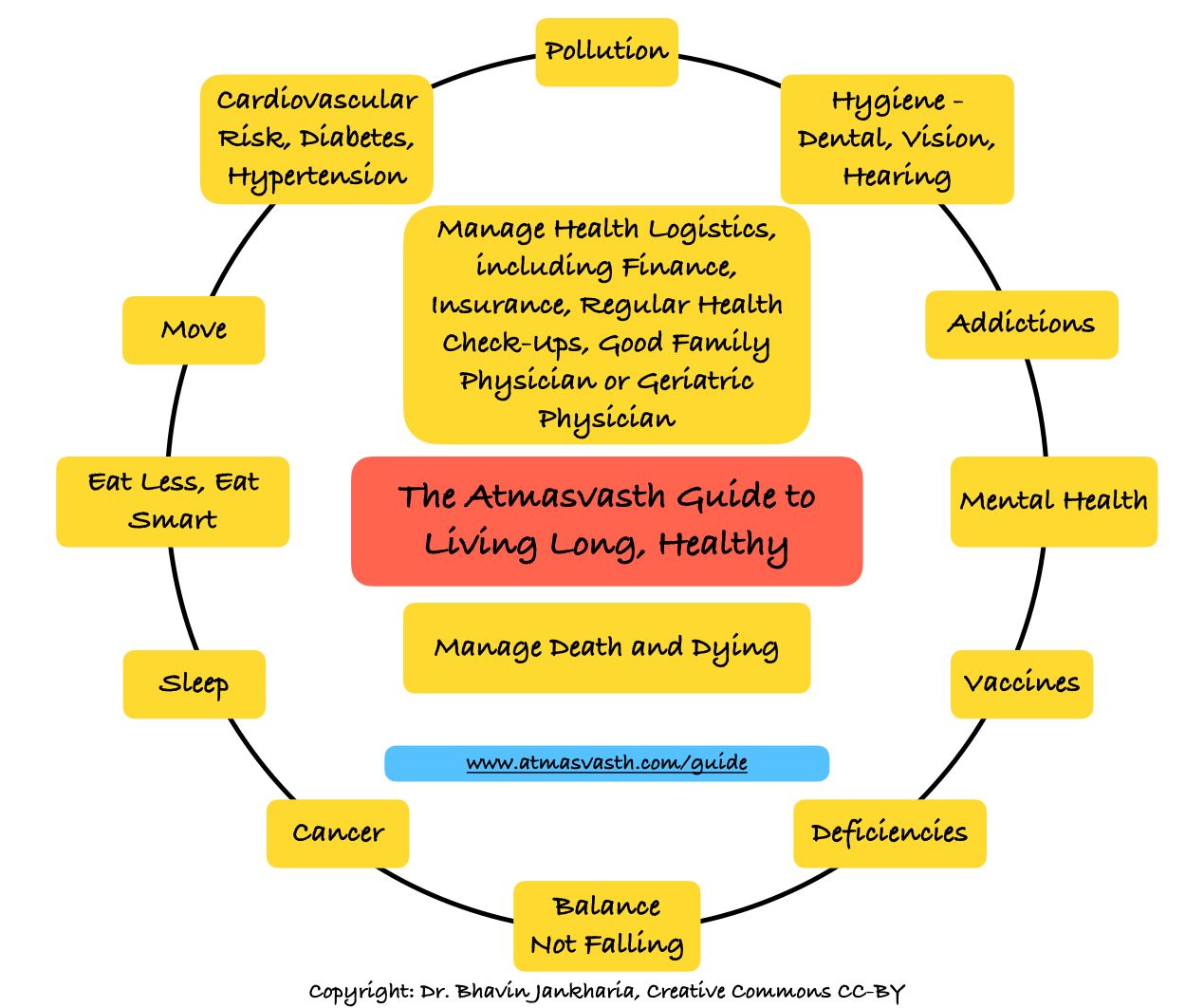
The 7th point in our atmasvasth guide to live, long healthy is
7. Do not fall (improve balance, take care not to fall) - daily and assess frailty - yearly
- Physical activity and strength training improve muscle and bone strength.
- Yoga and tai-chi help improve balance.
- Using walking aids like canes and walkers are double-edged swords - use them only if they can be monitored and only if absolutely necessary.
- Make sure you can see and hear well and avoid polypharmacy.
- Improve your household, building and other environmental factors to minimize falls…in effect, falls-proof your home and surroundings.
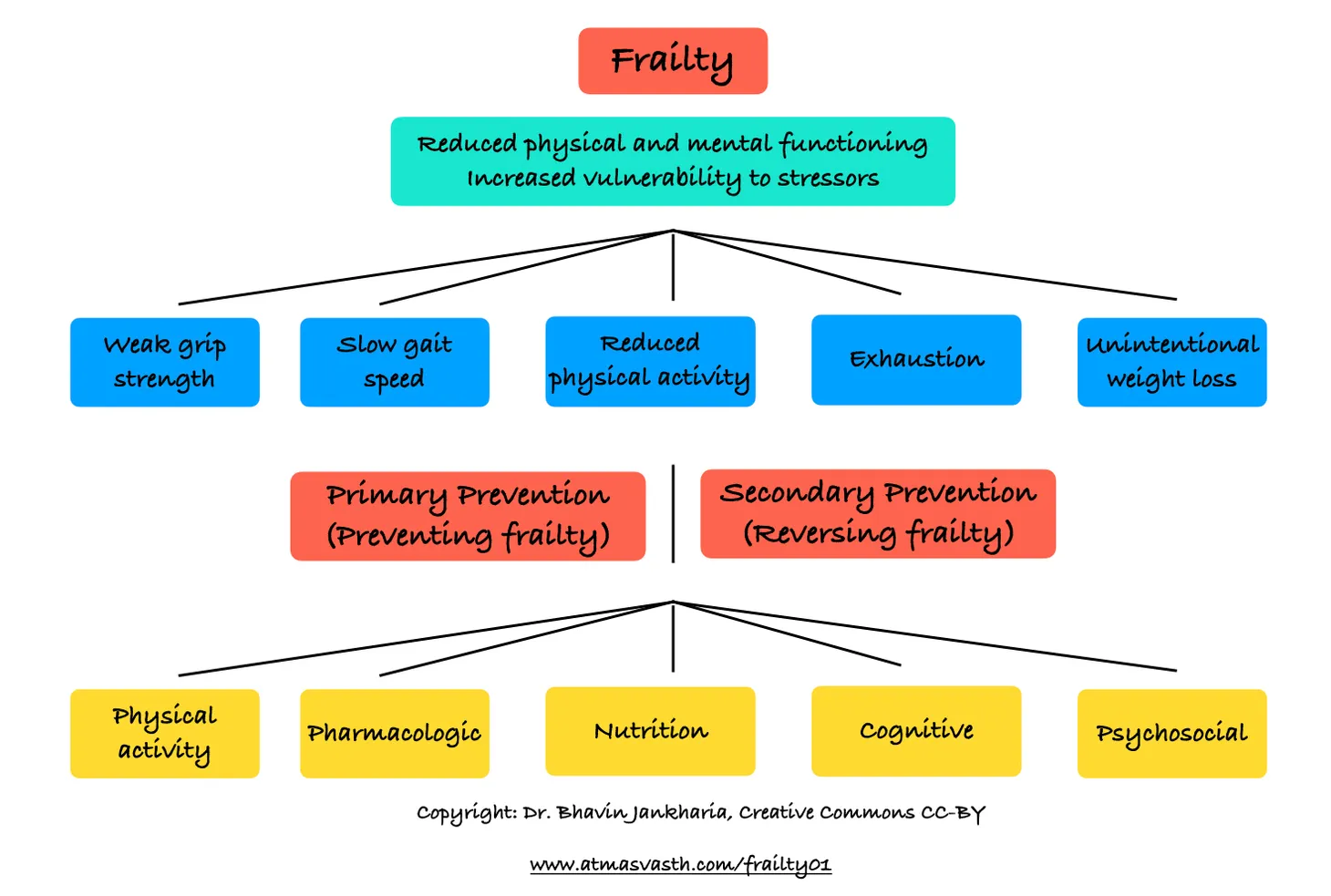
- Assess and manage frailty.
Many individuals as they age, lose muscle power and strength and slowly become less and less mobile and lose the ability to function independently. For years, this was considered a normal ageing process, but like osteoporosis and cognition loss, this is not normal and is preventable and sometimes reversible/controllable.
Many of you who care for people in their 70s and 80s may see this slow but inexorable physical decline that eventually requires the need for wheelchair assistance when traveling and the need for ward-boys or attendants to help with daily acts of living. Or you may be one of those who is going through this process.
It is important to understand the concept and to see what it is we can do to prevent muscle failure as we grow older and/or to control or reverse it, if it does occur.
Perhaps the first thing to understand is that while sarcopenia is a part of the definition of frailty, many who have sarcopenia and muscle failure are not necessarily frail. One of the challenges therefore is how to define sarcopenia [1]. Methods range from the hand-grip or sit-to-stand tests to visual assessment of walking quality and speed to the use of quantitative methods to measure muscle mass. All these have some pros and cons and therefore often a combination of these is used to identify patients who are at risk or have early muscle failure.
While a doctor may be able to figure this out, the challenge is that most doctors have no clue what sarcopenia/dynapenia or muscle failure is, which complicates the situation.
So, if you see someone around you slowing down, shuffling, walking slower than usual, needing support all the time, finding daily activities difficult, chances are the person has sarcopenia/muscle failure. You will then need to meet a doctor to rule out conditions like spinal problems, myositis, etc that can resemble sarcopenia. Once no other cause is found and the diagnosis gets established then you need to figure out what to do next to improve the situation.
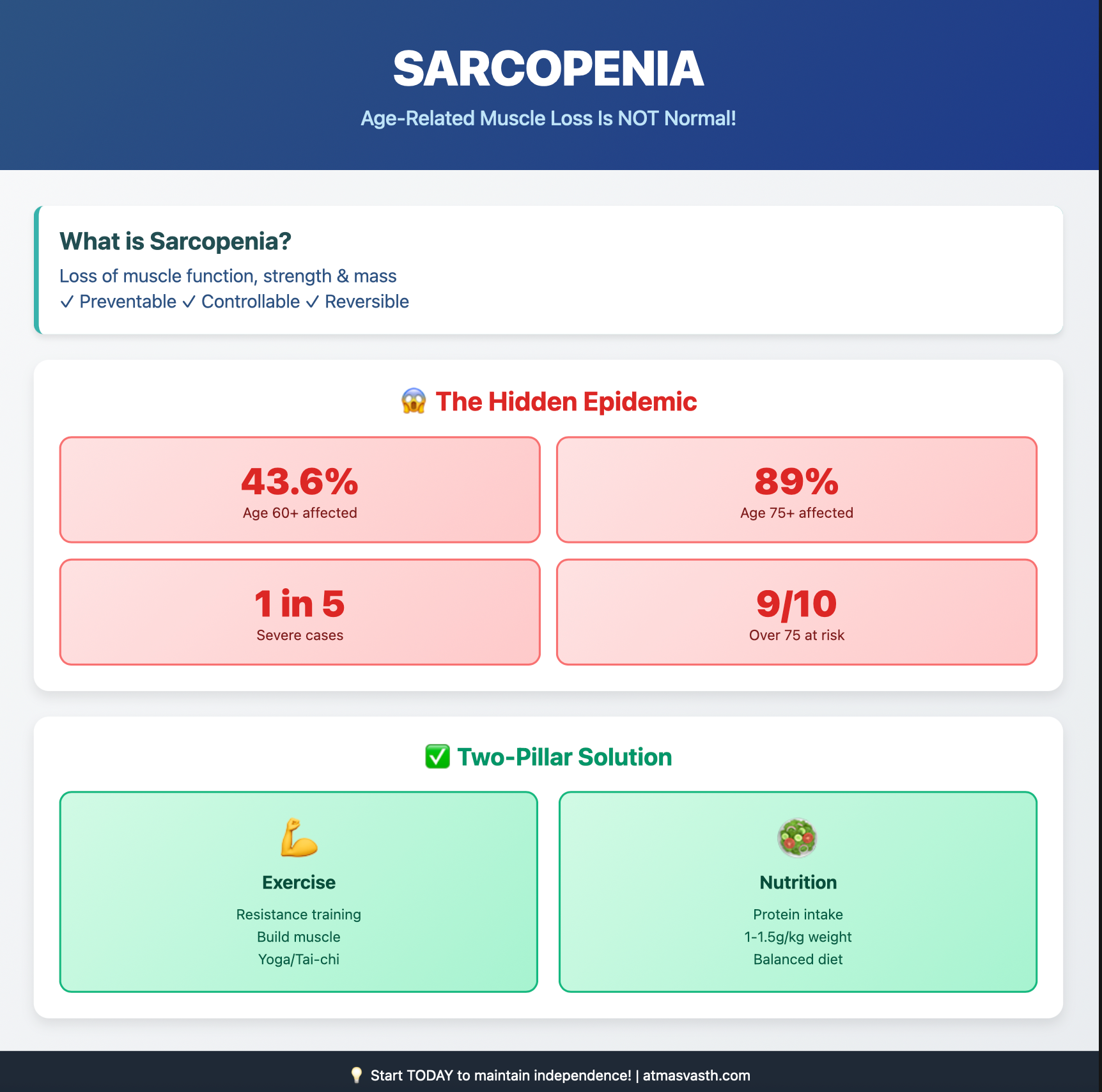
Why is this important? Because the problem is underdiagnosed, under-reported and ill-understood. A LASI dataset analysis recently showed that the prevalence of sarcopenia in those over 60 is 43.6% [2], which means pretty much every other person has some degree of muscle failure, which if not addressed, will only worsen and increase disability. Sarcopenia in the LASI study was diagnosed using handgrip strength, walking/gait speed and appendicular muscle mass based on sex, weight, height and age. 19% had severe sarcopenia, which is 1 in 5. Those over 75 were even worse off, with 89% having sarcopenia (9 out of 10 people over 75) with half of them having severe sarcopenia. These are crazy numbers.
While the LASI dataset includes people from all walks of life, it is likely that the numbers will be lower in those from a higher socioeconomic strata. However, even in the developed Western world, the prevalence varies from 5% to 17% to 43% depending on the definition used and the population studied.
There are recent Indian guidelines [3]. They define sarcopenia very simply as a decrease in muscle function, strength or mass. They recommend simple tests such as calf circumference, mid-upper arm circumference, handgrip strength and gait speed or the chair-stand test for a quick diagnosis.
The prevention of sarcopenia involves two main pillars - physical activity, mainly resistance training aimed at building up muscle and muscle resilience and adequate nutrition, especially protein intake.
The generation of Indians in India, currently in their late 70s and 80s was never aware of all this. Physical activity and muscle building were never part of their lifestyle and so when they hit an age where muscle failure starts to become common, they now find that there is no resilience to fall back upon. Similarly, conscious protein intake has never been part of our food culture, especially if you are vegetarian/vegan/Jain, etc and the challenges of a carb-fat predominant diet are now becoming evident later in life when you land up living longer.
Apart from resistance training and protein intake, the Indian guidelines mention supplements such as creatine, HMB and omega-3 fatty acids, but there are no international guidelines that currently support their use.
What does this mean for you and I?
If you see someone around you slowing down physically or you yourself are in that boat, you may have sarcopenia, with or without frailty. There is a dearth of doctors who understand the concept, so you will need to find someone who can examine you and confirm the diagnosis and rule out other causes for the loss of muscle strength, power and mobility. Once confirmed, the two main ways of managing sarcopenia are resistance training with a trainer or physiotherapist and adequate nutrition with at least 1 gm to 1.5 gm of protein per kg body weight. Additional supplements should be reserved for the time being until there is more data.
I will keep adding to the sarcopenia and muscle failure space as we know more.
Footnotes
1. Mathew RO et al. Performance of the American Heart Association’s PREVENT risk score for cardiovascular risk prediction in a multiethnic population. Nat Med. 2025 Aug;31(8):2655–62.
2. Saboo N, Rao A, Kacker S. The Effect of a Yoga Lifestyle on QRISK3 Score Among Individuals at High Risk for Cardiovascular Disease. Int J Yoga Therap. 2024 Nov 1;34(2024):Article 16. doi: 10.17761/2024-D-23-00055.
3. Pandey D, et al. Cardiovascular disease risk estimation among slums residents of Lucknow using QRISK3 calculator. J Educ Health Promot. 2025 Apr 30;14:149. doi: 10.4103/jehp.jehp_711_24.
Atmasvasth Newsletter
Join the newsletter to receive the latest updates in your inbox.
{kind=link}